
1
HP-2022-01
Access to Preventive Services without Cost-Sharing:
Evidence from the Affordable Care Act
Research examining the impact of the Affordable Care Act suggests that millions of
individuals have benefitted from increased access to care and coverage of clinical
preventive services without cost-sharing.
KEY POINTS
• The Affordable Care Act (ACA) substantially increased access to care and coverage of preventive
services without cost-sharing for millions of Americans.
• Many preventive services including vaccinations, well-child visits, screening for HIV and sexually
transmitted infections, HIV pre-exposure prophylaxis, contraception, and cancer screening are
required to be covered by most group and individual health plans and for many Medicaid
beneficiaries without cost-sharing.
• Expanded access to recommended preventive services resulted from increases in the number of
people covered through private health insurance and Medicaid expansion under the ACA.
• Analysis of recent data indicates that more than 150 million people with private insurance –
including 58 million women and 37 million children – currently can receive preventive services
without cost-sharing under the ACA, along with approximately 20 million Medicaid adult
expansion enrollees and 61 million Medicare beneficiaries that can benefit from the ACA’s
preventive services provisions.
• Evidence from studies examining the impact of the ACA indicate increased colon cancer
screening, vaccinations, use of contraception, and chronic disease screening.
BACKGROUND
Preventive services can help people avoid acute illness, identify and treat chronic conditions, prevent cancer or
lead to earlier detection, and improve health. The Affordable Care Act (ACA) reduced financial barriers to
accessing preventive services by requiring that most private health plans cover certain recommended
preventive services without cost-sharing. This requirement became effective for new health coverage
beginning on or after September 23, 2010, except for a requirement concerning women’s preventive services,
which became effective for plan years beginning on or after August 1, 2012.
January 11, 2022

JANUARY 2022
ISSUE BRIEF
2
Under the ACA, in most instances group health plans and individual health coverage plans cannot charge a
patient a copayment, co-insurance, or deductible for these services when they are delivered by an in-network
provider.
*
One exception are so-called “grandfathered” plans, which are plans that were in existence prior to
2010 and are allowed to continue offering benefit designs other than those generally required by the ACA. By
eliminating cost-sharing for these services, the ACA was designed to increase access and use of preventive
care, especially among individuals for whom affordability was a key barrier.
This issue brief summarizes the ACA’s preventive services provisions for private health coverage, Medicare,
and Medicaid; provides updated estimates of the number of people benefiting from these provisions
nationally; and examines evidence on trends in utilization of preventive services and outcomes since the ACA’s
preventive services coverage requirements went into effect.
POLICY OVERVIEW
Private Health Coverage
Under the ACA, most private insurance plans are required to cover four categories of preventive services in-
network without cost-sharing, including:
1. evidence-based preventive services that have in effect a rating of A or B in the current
recommendations of the U.S. Preventive Services Task Force (USPSTF), which indicates moderate to
high certainty that the net benefits of those services are moderate to substantial;
1
2. routine vaccines for adults and children that have in effect a recommendation from the Advisory
Committee on Immunization Practices (ACIP) and which has been adopted by the Director of the
Centers for Disease Control and Prevention (CDC);
2
3. evidence-informed preventive services for infants, children, and adolescents provided for in
comprehensive guidelines supported by the Health Resources and Services Administration (HRSA);
†
,3
and
4. preventive care and screenings for women, other than those that have in effect a rating of A or B in the
current recommendations of the USPSTF, that are provided for in comprehensive guidelines supported
by HRSA.
4
These requirements do not apply to grandfathered plans, which are plans that existed on March 23, 2010,
before the law was enacted, that meet certain requirements, and that are exempt from certain provisions of
the ACA.
‡
The range of preventive services covered without cost-sharing includes services such as alcohol misuse
screening and counseling, blood pressure screening, depression screening, immunizations, and obesity
screening and counseling. Certain covered preventive services recommended by the USPSTF are specific to
people in certain age groups or individuals at increased risk; for example, screening for latent tuberculosis in
populations at increased risk of infection, and colorectal cancer screening for adults aged 45 to 75.
5,6,7
The
USPSTF defers to the ACIP on recommendations concerning the use of vaccines.
§
_______________________
†
The guidelines implemented by HRSA are commonly referred to as Bright Futures and the Women’s Preventive Services Guidelines.
‡
These requirements also do not apply to coverage of certain services when a religious exemption applies.
§
The Centers for Disease Control and Prevention (CDC) sets the U.S. adult and childhood immunization schedules based on
recommendations from the ACIP.

JANUARY 2022
ISSUE BRIEF
3
Most health plans also generally must cover a set of preventive services for children without cost-sharing (i.e.,
those plans that are not grandfathered as discussed above) including those providing coverage in the group,
individual, and Medicaid markets.
8
Preventive services benefits for children include, but are not limited to,
alcohol, tobacco, and drug use assessments for adolescents; universal newborn hearing screening;
developmental and autism screening for children at 18 and 24 months; bilirubin concentration screening for
newborns; blood pressure screening for children ages 0 to 17 years; developmental screening for children
under age 3; and routine immunization for children from birth to age 18 (doses, recommended ages, and
recommended populations vary).
In most instances, non-grandfathered group and individual health coverage plans are required to cover certain
preventive benefits for women, including well-woman visits, screening and counseling for domestic violence,
U.S. Food and Drug Administration (FDA)-approved contraceptive methods, and other services specified in the
Women's Preventive Services Guidelines, which initially went into effect August 2012.
9
These guidelines are
updated periodically to reflect the latest evidence-based recommendations including, for example, a
recommendation that adolescent and adult women have access to the full range of FDA-approved
contraceptive products, effective family planning practices, and sterilization procedures for women to prevent
unintended pregnancy and improve health outcomes.
Estimated Population Size with Private Health Coverage Benefitting from ACA Provisions
Previous analyses by the Office of the Assistant Secretary for Planning and Evaluation (ASPE) estimated that
approximately 137 million Americans with private insurance had access to preventive services without cost
sharing in 2015.
10,
**
Using the same method, ASPE estimates that about 151.6 million had such coverage in
2020. The increase is due in part to growth in the number of people enrolled in private health coverage and a
decrease in the share of such people enrolled in grandfathered plans.
In 2020, the most recent year of data available, 175.9 million people under age 65 had private health coverage,
mainly through an employer, but also including coverage purchased through a state or federal Marketplace.
11
The 2020 Kaiser Family Foundation Employer Health Benefits survey found that 14 percent of individuals with
employer-based health plans were enrolled in grandfathered plans, which are not required to provide
preventive service coverage with zero cost-sharing (we assume that these individuals are subject to some level
of cost sharing for preventive services). Data from the 2020 Final Rule on Grandfathered Health Plans and from
the 2020 National Health Expenditures Accounts suggest that at most 12 percent of people with individual
market coverage are enrolled in grandfathered health plans.
††
Using these statistics, we estimate that a total
of approximately 151.6 million individuals
12
currently have private health coverage that covers preventive
services with zero cost-sharing (Figure 1).
13
This includes approximately 58 million women, 57 million men,
and 37 million children. Table 1 presents state-level estimates.
_______________________
**
ASPE released a different estimate in 2012 focused on the number of people newly gaining coverage for free preventive services,
based on how many people with private coverage already had access to preventive care vs. how many were gaining it for the fir st time,
with an estimate of 54 million. The more recent reports, including this report, provide estimates of how many total people have private
coverage without cost-sharing for these services, whether or not some may have had similar coverage prior to the ACA.
††
See Figure 1 sources for more information on this estimate.

JANUARY 2022
ISSUE BRIEF
4
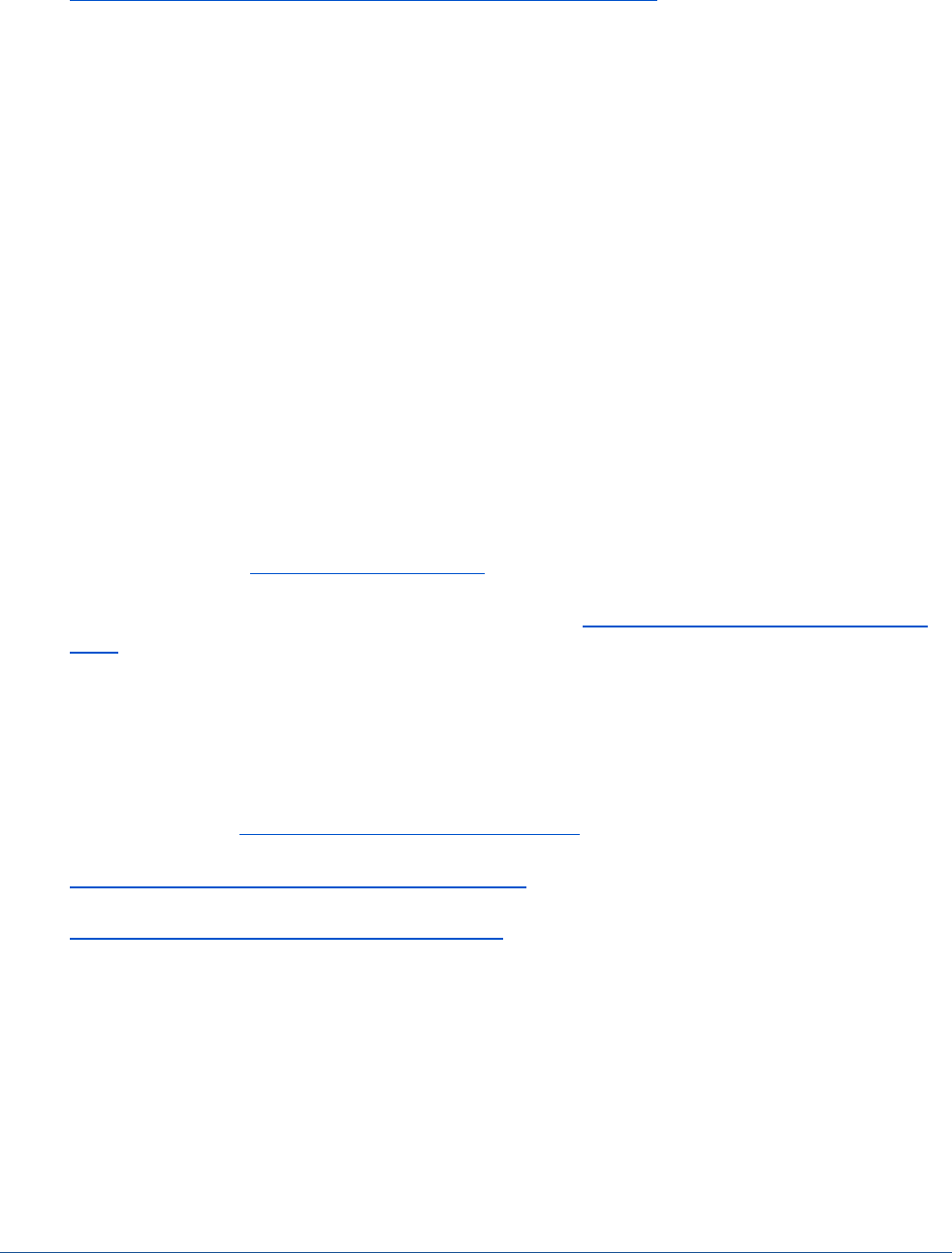
Figure 1.Estimated Number of Individuals with Private Health Coverage, by
Age and Gender, with Preventive Services Coverage without Cost-
Sharing, 2020 (in millions)
Note: ASPE subtracted estimated 14% and 12% of grandfathered plan enrollees from the total
number of individuals with employee sponsored health insurance and the total number of
individuals with nongroup insurance, respectively, to estimate the number of privately covered
individuals with preventive services coverage without cost-sharing.
Sources: Privately insured individuals, by age and gender: 2020 Kaiser Family Foundation State
Health Facts on Health Coverage and the Uninsured, developed from the 2017-2021 Current
Population Survey (CPS) Annual Social and Economic Supplements: https://www.kff.org/state-
category/health-coverage-uninsured/
Grandfathered plan estimates: 2020 Kaiser Family Foundation Employer Health Benefits Survey:
https://www.kff.org/health-costs/report/2020-employer-health-benefits-survey/
Non group estimate calculated from 2020 Final Rule on Grandfathered Health Plans and 2020 National Health
Expenditures Table 22 on coverage:
https://www.govinfo.gov/content/pkg/FR-2020-12-15/pdf/2020-27498.pdf
https://www.cms.gov/Research-Statistics-Data-and-Systems/Statistics-Trends-and-
Reports/NationalHealthExpendData/NationalHealthAccountsHistorical
37.1
58.0
56.5
151.6
0
20
40
60
80
100
120
140
160
Children 0-18 Women 19-64 Men 19-64 Total
Number of Americans
(in millions)

JANUARY 2022
ISSUE BRIEF
5
Table 1. State-level Estimates of Individuals with Private Health
Coverage with Preventive Services Coverage without Cost-Sharing, 2020
(in thousands)
Children
(<19)
Women
(ages 19-64)
Men
(ages 19-64)
Total
United States
37,077
58,019
56,483
151,579
Alabama
513
813
757
2,084
Alaska
60
95
91
246
Arizona
758
1,121
1,163
3,042
Arkansas
274
480
460
1,214
California
4,411
6,718
6,860
17,988
Colorado
625
1,032
1,055
2,712
Connecticut
341
615
587
1,543
Delaware
92
174
153
420
District of Columbia
53
157
156
367
Florida
1,872
3,606
3,566
9,045
Georgia
1,081
1,871
1,706
4,658
Hawaii
134
229
236
599
Idaho
227
315
320
862
Illinois
1,656
2,429
2,433
6,518
Indiana
946
1,241
1,220
3,407
Iowa
406
588
593
1,587
Kansas
402
523
517
1,441
Kentucky
414
712
713
1,840
Louisiana
417
663
644
1,724
Maine
105
248
220
573
Maryland
800
1,195
1,118
3,113
Massachusetts
767
1,326
1,249
3,343
Michigan
1,203
1,759
1,697
4,659
Minnesota
817
1,145
1,135
3,097
Mississippi
294
513
445
1,252
Missouri
741
1,152
1,070
2,964
Montana
116
171
166
453
Nebraska
278
364
388
1,030
Nevada
316
524
529
1,369
New Hampshire
162
261
279
702
New Jersey
1,143
1,673
1,693
4,509
New Mexico
131
257
251
640
New York
2,073
3,452
3,067
8,592
North Carolina
959
1,908
1,783
4,650
North Dakota
114
141
156
411
Ohio
1,302
1,983
1,950
5,235
Oklahoma
379
578
579
1,537
Oregon
510
803
740
2,053
Pennsylvania
1,432
2,441
2,348
6,220
Rhode Island
127
206
191
524
South Carolina
483
887
905
2,275
South Dakota
113
163
174
450
Tennessee
685
1,118
1,093
2,895
Texas
3,472
4,884
4,583
12,939
Utah
617
620
591
1,829
Vermont
64
114
115
292
Virginia
1,115
1,680
1,596
4,392
Washington
896
1,502
1,477
3,875
West Virginia
172
277
294
743
Wisconsin
704
1,191
1,276
3,171
Wyoming
62
101
93
256
Note: ASPE subtracted the estimated 14% and
12% of grandfathered plan enrollees from the
total number of individuals with employee
sponsored health insurance and the total number
of individuals with nongroup insurance,
respectively, to estimate the number of privately
covered individuals with preventive services
coverage without cost-sharing. Numbers of
individual children, women, and men may not
sum to total due to rounding.
Sources: Privately insured individuals, by age and
gender: 2020 Kaiser Family Foundation State Health
Facts on Health Coverage and the Uninsured,
developed from the 2017-2021 Current Population
Survey (CPS) Annual Social and Economic
Supplements: https://www.kff.org/state-
category/health-coverage-uninsured/
Grandfathered plan estimates: 2020 Kaiser Family
Foundation Employer Health Benefits Survey:
https://www.kff.org/health-costs/report/2020-
employer-health-benefits-survey/
Non group adjustment calculated from 2020 Final
Rule on Grandfathered Health Plans and 2020
National Health Expenditures Table 22 on coverage:
https://www.govinfo.gov/content/pkg/FR-2020-12-
15/pdf/2020-27498.pdf
https://www.cms.gov/Research-Statistics-Data-and-
Systems/Statistics-Trends-and-
Reports/NationalHealthExpendData/NationalHealthA
ccountsHistorical

JANUARY 2022
ISSUE BRIEF
6
Medicaid and Children’s Health Insurance Program
In addition to the 151.6 million individuals with non-grandfathered group health plans and non-grandfathered
group and individual health coverage who benefit from preventive services coverage under the ACA, the ACA
provisions also address coverage of preventive services in both Medicare and Medicaid. Medicaid coverage
offered by states (and the District of Columbia) that have expanded Medicaid eligibility to non-elderly adults
with family incomes at or below 133 percent of the federal poverty level must cover the full range of
preventive services required by the essential health benefits (EHB) regulations, which includes recommended
preventive services coverage without cost-sharing.
In Medicaid, the ACA requirement for coverage of preventive services without cost-sharing applies only to
Medicaid expansion enrollees and other Medicaid enrollees in Alternative Benefit Plans. As of October 2021,
38 states and the District of Columbia have expanded Medicaid.
14
Under Medicaid expansion, approximately
20 million adults had coverage for preventive services without cost-sharing as of September 2021.
15
Unrelated to the ACA, all children in Medicaid (31 million in December 2020)
16
are covered without cost-
sharing for Early and Periodic Screening, Diagnostics and Treatment (EPSDT), created in 1967, which includes
well-child visits and ACIP-recommended vaccines,
17
and other essential preventive health benefits for children.
Medicaid coverage of preventive services for adults in states that have not expanded Medicaid is a state
option, but most states provided some level of coverage of these services before the ACA.
18
Tobacco cessation
for pregnant women is the only preventive service listed under mandatory Medicaid benefits.
19
Optional
benefits include “other diagnostic, screening, preventive and rehabilitative services.” In traditional Medicaid,
states that opt to cover all USPSTF Grade “A” or “B” recommended preventive services and ACIP-
recommended vaccines and their administration without cost-sharing receive a one percentage point increase
in the federal medical assistance percentage (FMAP) for those services.
20
State Medicaid Agencies are
encouraged to consider this option to ensure access to preventive services without cost-sharing to additional
Medicaid beneficiaries without mandatory coverage.
A total of 33 states covered well-adult exams in FFS and in managed care, and five states covered well-adult
exams in managed care in 2012.
21
Half the states charged co-pays in 2012. Three states did not cover
screening mammograms at all, and two states did not cover Pap testing while some states covered Pap testing
only as part of family planning visits. A 2018-19 study showed that only 24 out of 49 Medicaid state programs
responding to a survey covered all 13 ACIP-recommended adult vaccines.
22
A total of 48 Medicaid state FFS
programs covered hepatitis B and meningococcal ACWY
‡‡
vaccines and 47 Medicaid state FFS programs
covered influenza; tetanus, diphtheria, and pertussis (Tdap); measles, mumps, and rubella (MMR); varicella;
and pneumococcal vaccines. A total of 29 states out of 34 states responding to the survey required their
Medicaid managed care plans to cover Tdap, hepatitis B, and meningococcal ACWY vaccines, and 28 states
required their Medicaid Managed plans to cover influenza, MMR, varicella, pneumococcal conjugate, and
meningococcal B vaccines.
The Children’s Health Insurance Program (CHIP) is a program funded by the Federal government and states to
cover children up to age 19 in households with income too high to qualify for Medicaid. Ten states and the
District of Columbia cover all of their CHIP beneficiaries under Medicaid and provide them with the same
Medicaid benefits, including EPSDT.
23
Thirty-eight states cover some CHIP beneficiaries under Medicaid and
some under a separate CHIP program. Two states only have separate CHIP programs. All CHIP programs are
required to cover well-child visits without cost-sharing.
24
CHIP programs are also required to cover vaccines
_______________________
‡‡
Meningococcal ACWY vaccine can help protect against meningococcal disease caused by serogroups A, C, W, and Y.

JANUARY 2022
ISSUE BRIEF
7
and vaccine administration for children without cost-sharing. Fifteen states cover pregnant women under
CHIP.
25
The American Rescue Plan Act (ARP) requires CHIP programs to cover COVID-19 vaccines for children
and pregnant women without cost-sharing through the last day of the quarter of the end of the public health
emergency.
26
Other preventive services may be covered with or without cost-sharing by separate state CHIP
programs, but there are no studies on this. All children enrolled in CHIP (6.7 million in December 2020)
27
are
covered for vaccines and well-child visits without cost-sharing and may be covered for other preventive
services with or without cost-sharing.
Medicare
Under the ACA, services recommended by the USPSTF with a Grade “A” or “B” must be covered by Medicare
without cost-sharing if the Secretary of the U.S. Department of Health and Human Services (HHS) determines
through the national coverage determination process that they are reasonable and necessary for the
prevention or early detection of an illness or disability, and appropriate for individuals entitled to the
program’s Part A benefits or who are enrolled in Part B.
28
There are approximately 61.5 million individuals
enrolled in Medicare, all of whom potentially benefit from this provision of the ACA.
29
After the ACA was enacted, HHS issued new rules on November 29, 2010, to eliminate Medicare cost-sharing
for USPSTF recommended preventive services and to provide Medicare coverage for an annual wellness visit
that includes a comprehensive health risk assessment and a 5- to 10-year personalized prevention plan.
Medicare Part B provides coverage without cost-sharing for certain USPSTF-recommended services and four
vaccinations: COVID-19, influenza, hepatitis B, and pneumococcus. Medicare Part B does not currently cover
preventive shingles and tetanus, diphtheria, and pertussis (Tdap) vaccinations.
30
Optional Medicare Part D
plans generally cover these other vaccinations, though they may include cost-sharing.
§§
,31
The Build Back
Better Act (BBB), being considered in the Congress, proposes covering these vaccinations without cost-sharing
in Medicare Part D.
EVIDENCE ON CHANGES IN UTILIZATION AND OUTCOMES
Research shows that the ACA reduced health coverage disparities across racial groups and expanded access to
a range of clinical services including preventive services.
32,33
Gains in access to services were due in large part
to uninsured individuals obtaining health coverage. For example, people who became newly covered under
Medicaid and the Marketplace through the ACA in 2014 were much less likely than uninsured people to report
being unable to get care or delaying needed care because of cost.
34
There have been fewer studies specifically
examining the effects of eliminating cost-sharing for preventive services among individuals who already had
health coverage. In this section, we describe the effects of the ACA on utilization of several types of preventive
services; these effects are likely a combined result of the provisions expanding coverage to the uninsured and
the provisions increasing access to preventive services without cost-sharing.
Cancer Screening
Overall, Americans utilize recommended clinical preventive services at low rates, and utilization of preventive
services such as cancer screening differs across racial and ethnic populations.
35,36,37
ACA provisions to
eliminate cost-sharing for recommended clinical preventive services, such as cancer screenings, presented an
opportunity to increase early diagnosis of cancer. Studies examining changes in cancer screening among
privately insured individuals after the ACA eliminated cost-sharing show an overall increase in colorectal
cancer screening tests, while breast cancer screening rates were stable; rates of Pap testing decreased, though
_______________________
§§
Generally, Medicare prescription drug plans (Part D) cover all commercially available vaccines (e.g., shingles) needed to prevent illness.

JANUARY 2022
ISSUE BRIEF
8
this time period coincided with revised cervical cancer screening recommendations that include less frequent
testing for many patients.
38,39
An analysis of 2013-2016 national survey data indicated utilization rates among
newly insured immigrants increased for colon cancer screenings but did not change for Pap testing or
mammography.
40
Some research also shows that patient navigation interventions have helped increase
cervical cancer screening rates among Latinas and Chinese-American women.
41
While the studies reviewed
show some evidence of improved use of cancer screening since enactment of the ACA, disparities remain.
42,43
The USPSTF announced a new recommendation in May 2021 that colon cancer screening start at age 45
instead of 50.
44
We estimate that this means an additional 15.0 million to 17.5 million individuals will be able
to benefit from the ACA’s provisions for preventive services without cost-sharing for colon cancer screening.
45
An analysis of data from 2009 and 2014 suggest that the elimination of cost-sharing under the ACA positively
affected colorectal cancer screening among men and women with private health coverage, and among men
and Hispanic beneficiaries with Medicare coverage.
46
While data show that colon cancer mortality among men
and women was decreasing prior to the ACA, colon cancer remains one of the leading causes of cancer deaths,
and increased screening – which can result in identification and removal of precancerous growths – has
resulted in a decrease in colorectal cancer incidence.
47
Health coverage is important for individuals with cancer because access to care can affect health outcomes.
Annual out-of-pocket costs among recently diagnosed survivors of cancers like breast, prostate, colorectal, and
lung cancers average more than $1,000 for medical care costs, depending on age.
48
Some research suggests
that increased access to preventive services and increased affordability of care since the ACA has helped
cancer survivors obtain the care they needed.
49,50
However, decreases in cancer screenings during 2020 as a
result of the COVID-19 pandemic indicate the need to monitor post-pandemic changes in cancer incidence,
later-stage cancer diagnosis, and cancer mortality.
51,52
Vaccinations
One ACA provision with particular relevance for young adults is the dependent coverage provision, which
generally allows young adults to stay on their parents’ health care plans until age 26. With the ACA dependent
coverage provision and the provision for preventive services without cost-sharing, an estimated 854,000 young
women completed the human papillomavirus (HPV) vaccine series from 2010 to 2012, an increase of 5.8
percentage points compared to a control group of women who were not eligible for dependent coverage.
53
Coverage without cost-sharing was associated with a 4.3 percentage point increase in HPV vaccine completion
for females aged 9 to 26 who were privately insured and a 5.7 percentage point increase for Medicaid
enrollees in three states (Massachusetts, New Hampshire, and Maine) in a study of 2009-2015 claims.
54
Influenza vaccinations showed a small but significant increase from 2009 to 2011/2012 after the elimination of
cost-sharing among adults with private health coverage.
55
National survey data from 2016 showed that among
adults 65 and older, 70.4 percent received an influenza vaccine and 66.9 percent had been vaccinated against
pneumococcal disease; Tdap vaccination of adults 19 years and older was just 26.6 percent.
56
Thus, many
adults do not receive all of the recommended vaccinations, sometimes for reasons other than cost, and there
is still potential for greater uptake and utilization of routine vaccination among adults who have private health
coverage, Medicare, and Medicaid.
57
Medicare Wellness Visits
The percentage of Medicare beneficiaries utilizing annual wellness visits increased 14.9 percentage points
between 2011 (the first year when such visits were covered) and 2016, rising from 8.1 percent to 23.0
percent.
58
This trend suggests that it may take time for beneficiaries and providers to use a new service when
it becomes available. However, the utilization of this new service was characterized by disparities, with

JANUARY 2022
ISSUE BRIEF
9
utilization 10.2 percentage points lower for non-Hispanic Black Medicare beneficiaries and 11.6 percentage
points lower for Hispanic beneficiaries than non-Hispanic White beneficiaries in 2016.
Women’s Health and Contraception
Provisions in the ACA addressed a range of women’s health needs by increasing health coverage – which
increased access to medical and mental health care – and by establishing HRSA-supported Women's
Preventive Services Guidelines specifying certain services that must be covered without cost-sharing by non-
grandfathered group and individual health coverage. Services included in the Women’s Preventive Services
Guidelines are: screening for anxiety, breast cancer screening for average-risk women, breastfeeding services
and supplies, screening for cervical cancer, contraception (including contraceptive counseling), screening for
gestational diabetes mellitus, screening for diabetes after pregnancy, screening for human immunodeficiency
virus infection, screening for interpersonal and domestic violence, counseling for sexually transmitted
infections, well-woman preventive visits, and screening for urinary incontinence.
Most recently in January 2022, the Guidelines incorporated new, updated evidence-based recommendations
for breastfeeding services and supplies, contraception, screening for human immunodeficiency virus (HIV)
infection, counseling for sexually transmitted infections, and well-woman preventive visits, and added a new
recommendation for preventing obesity in midlife women.
Access to contraceptives has been shown to improve a variety of women’s health and economic outcomes,
including reduced rates of entry into poverty, increased rates of entry into professional school, or the labor
force, and increases in wages.
59,60
Access has also had intergenerational effects. Children of women who have
access to contraceptives have been shown to achieve higher rates of college graduation and higher incomes
than children of women who did not have access to contraceptives.
61
Contraceptives include a wide array of
products. Long-acting reversible contraceptives (LARCs) – which include intrauterine devices (IUDs),
intrauterine systems (IUSs), and subdermal implants – are among the most effective methods of
contraception, while the birth control pill is among the most popular. Other types of contraception include the
hormone patch, the vaginal ring, and emergency contraceptive medication. The ACA provision requiring
coverage of contraceptives without cost-sharing mitigated a major barrier to contraceptive use: cost. High
cost-sharing has been shown to be associated with contraceptive nonadherence and discontinuation, as well
as lower use of LARCs, which often have high one-time costs even though they can be less expensive over time
than methods that must be purchased periodically such as the birth control pill.
62,63,64,65
A comparison of out-of-pocket costs for contraception before and after the implementation of the ACA found
that average costs for every category of contraception decreased. The mean out-of-pocket cost for an IUD fell
from $262.38 in the first half of 2012 to $84.30 in the first half of 2013. The ACA provision saved an average of
$255 annually per user of birth control pills between 2012 and 2013.
66
After the implementation of the ACA’s
preventive service zero-cost sharing requirements, the median out-of-pocket spending for all categories except
the vaginal ring and the subdermal patch was $0. The estimated out-of-pocket savings to women totaled
approximately $1.4 billion in 2013.
Research also demonstrates that the reduction in cost-sharing led to increased use of LARCs. One study found
that the reduction in cost-sharing was associated with increases in prescription contraceptive usage, with a
shift toward longer-term methods (including non-reversible options such as sterilization).
67
A later study found
that women enrolled in high deductible health plans (HDHPs) initiated LARC use at rates more than twice as
high than women in non-high deductible health plans (non-HDHPs) beginning after the implementation of the
ACA. This study is consistent with the idea that women in HDHPs were hesitant to access IUDs/LARCs because
they would have had higher cost-sharing due to their high deductibles, until the ACA provision removed that
barrier.
68

JANUARY 2022
ISSUE BRIEF
10
An analysis of data through 2018 showed that ACA Medicaid expansion was associated with greater
preconception health counseling and postpartum use of effective birth control methods among low-income
women, and another study found that expanded Medicaid coverage under the ACA was associated with
decreases in the proportion of pregnancies that were unintended among individuals with a high-school degree
or less, but was not associated with any significant change in the overall birth rate.
69,70
The overall national
rate of intended pregnancy decreased from 67 percent of births to 62 percent of births between 2011 and
2019.
***
,71
Chronic Conditions
Gaining access to health coverage and preventive services can allow earlier detection and treatment of chronic
health conditions such as hypertension and diabetes. Several studies have found that the ACA resulted in
improvements in affordability of care, regular care for chronic conditions, medication adherence, and self-
reported health.
72,73
During 2012-2015, the percentage of adults aged 18 to 64 with two or more chronic
health conditions who delayed or did not obtain needed medical care due to cost decreased.
74
More adults with private insurance received blood pressure and cholesterol screening in 2011-12, compared to
pre-ACA screening rates in 2009.
75
An analysis of 2012-2018 data showed that ACA Medicaid expansion was
associated with sustained increases in improvements in blood pressure and glucose control over a five-year
period among individuals receiving care at Federally Qualified Health Centers, especially Black and Hispanic
patients.
76
Preventive services and chronic disease management contribute to improvements in cardiovascular
health, blood pressure control,
77
and both the incidence and care for diabetes; increasing access to such
services is an important factor in improving health outcomes over time and addressing health disparities. ACA
implementation has also contributed to improved health outcomes among people living with HIV in terms of
viral suppression and retention in care.
78
CONCLUSIONS
The implementation of the ACA increased health coverage, especially among Black Americans, Latinos, Asian
Americans and Pacific Islanders, American Indians/Alaska Natives, and individuals living in states that
expanded Medicaid.
79,80,81,82
We estimate that more than 150 million people with private health coverage are
now benefitting from the ACA’s coverage of preventive services without cost-sharing, across a range of
services and conditions. In addition, tens of millions of Medicare and Medicaid beneficiaries are also
benefitting from the ACA provisions regarding preventive services without cost-sharing. Studies demonstrate
increases in access to preventive services, including colon cancer screening, HPV vaccination, Medicare annual
wellness visits, and contraceptive use. Investments in prevention in the early and middle decades of life, when
people are more likely to be covered by private health coverage including Marketplace insurance and
Medicaid, may also help people enter the Medicare program at age 65 in better health. Ongoing research can
help monitor the impact of the ACA on access to care, use of preventive services, health disparities, and long-
term health outcomes.
_______________________
***
Intendedness of births as reported by women, 2011-2015 and 2017-2019 National Survey of Family Growth data

JANUARY 2022
ISSUE BRIEF
11
REFERENCES
1. The Patient Protection and Affordable Care Act, Sec. 2713 (a)(1)
2. The Patient Protection and Affordable Care Act, Sec. 2713 (a)(2)
3. The Patient Protection and Affordable Care Act, Sec. 2713 (a)(3)
4. The Patient Protection and Affordable Care Act, Sec. 2713 (a)(4)
5. U.S. Preventive Services Task Force. Latent Tuberculosis Infection: Screening.
https://www.uspreventiveservicestaskforce.org/uspstf/index.php/recommendation/latent-
tuberculosis-infection-screening
6. U.S. Preventive Services Task Force. Colorectal Cancer: Screening.
https://www.uspreventiveservicestaskforce.org/uspstf/index.php/recommendation/colorectal-cancer-
screening
7. Centers for Medicare & Medicaid Services. Preventive care benefits for adults.
https://www.healthcare.gov/preventive-care-adults/
8. Centers for Medicare & Medicaid Services. Preventive care benefits for children.
https://www.healthcare.gov/preventive-care-children/
9. Health Resources and Services Administration. Women's Preventive Services Guidelines.
https://www.hrsa.gov/womens-guidelines/index.html
10. ASPE. The Affordable Care Act is Improving Access to Preventive Services for Millions of Americans.
https://aspe.hhs.gov/reports/affordable-care-act-improving-access-preventive-services-millions-
americans
11. Census Bureau. Health Insurance Coverage in the United States: 2020.
https://www.census.gov/content/dam/Census/library/publications/2021/demo/p60-274.pdf
12. Sum of Men 19-64, Women 19-64, Children 0-18 with employer-sponsored, nongroup, or TRICARE
insurance, 2020 Kaiser Family Foundation State Health Facts on Health Coverage and the Uninsured,
based on the 2017-2021 Current Population Survey (CPS) Annual Social and Economic Supplements:
https://www.kff.org/state-category/health-coverage-uninsured/ Adjustments based on 2020 Kaiser
Family Foundation Employer Health Benefits Survey: https://www.kff.org/health-costs/report/2020-
employer-health-benefits-survey/
13. ASPE. The Affordable Care Act is Improving Access to Preventive Services for Millions of Americans.
https://aspe.hhs.gov/pdf-report/affordable-care-act-improving-access-preventive-services-millions-
americans
14. U.S. Department of Health and Human Services. Missouri Medicaid Expansion Brings Quality Essential
Health Coverage to More than 275,000 Missourians. October 4, 2021.
https://www.hhs.gov/about/news/2021/10/04/missouri-medicaid-expansion-brings-quality-essential-
health-coverage.html
15. Centers for Medicare & Medicaid Services internal enrollment data for September 2021
16. Centers for Medicare & Medicaid Services. December 2020 and January 2021 Medicaid and CHIP
Enrollment Trend Snapshot. https://www.medicaid.gov/medicaid/national-medicaid-chip-program-
information/downloads/december-2020-january-2021-medicaid-chip-enrollment-trend-snapshot.pdf
17. Centers for Medicare and Medicaid. Early and Periodic Screening, Diagnostics, and Treatment.
https://www.medicaid.gov/medicaid/benefits/early-and-periodic-screening-diagnostic-and-
treatment/index.html
18. Wilensky S and Gray S. Coverage of Medicaid Preventive Services for Adults – A National Review.
Prepared for the American Cancer Society, the American Cancer Society Cancer Action Network, the
American Heart Association and the National Colorectal Cancer Roundtable, November 2012.
19. Section 1905(a)(4)(D) of the Social Security Act; see Centers for Medicare & Medicaid Services.
Mandatory & Optional Medicaid Benefits. https://www.medicaid.gov/medicaid/benefits/mandatory-
optional-medicaid-benefits/index.html
JANUARY 2022
ISSUE BRIEF
12
20. Section 1905(b)(5) of the Social Security Act; see Centers for Disease Control and Prevention. High
Quality Care: Access and Delivery - Preventive Services Coverage.
https://www.cdc.gov/nchhstp/highqualitycare/preventiveservices/
21. Wilensky S and Gray S. Coverage of Medicaid Preventive Services for Adults – A National Review.
Prepared for the American Cancer Society, the American Cancer Society Cancer Action Network, the
American Heart Association and the National Colorectal Cancer Roundtable, November 2012.
22. Granade C et al. State Policies on Access to Vaccination Services for Low-Income Adults. JAMA
Network Open, April 27, 2020.
23. Centers for Medicare & Medicaid Services. CHIP Program Structure by State.
https://www.medicaid.gov/chip/downloads/chip-map.pdf
24. Centers for Medicare & Medicaid Services. CHIP Benefits.
https://www.medicaid.gov/chip/benefits/index.html
25. Kaiser Family Foundation, March 2021. Medicaid and CHIP Eligibility and Enrollment Policies as of
January 2021: Findings from a 50-State Survey. https://files.kff.org/attachment/Report-Medicaid-and-
CHIP-Eligibility-and-Enrollment-Policies-as-of-January-2021-Findings-from-a-50-State-Survey.pdf
26. Centers for Medicare & Medicaid, May 5, 2021. Coverage and Reimbursement of COVID-19 Vaccines,
Vaccine Administration, and Cost Sharing under Medicaid, the Children’s Health Insurance Program,
and Basic Health Program. https://www.medicaid.gov/state-resource-center/downloads/covid-19-
vaccine-toolkit.pdf
27. Centers for Medicare & Medicaid Services. December 2020 and January 2021 Medicaid and CHIP
Enrollment Trend Snapshot. https://www.medicaid.gov/medicaid/national-medicaid-chip-program-
information/downloads/december-2020-january-2021-medicaid-chip-enrollment-trend-snapshot.pdf
28. https://www.cms.gov/Research-Statistics-Data-and-Systems/Statistics-Trends-and-
Reports/Beneficiary-Snapshot/Bene_Snapshot
29. 42 USC 1395x(ddd). https://uscode.house.gov/
30. Centers for Medicare & Medicaid Services. Preventive and Screening Services. www.medicare.gov
31. Centers for Medicare & Medicaid Services. Shingles Shots. www.medicare.gov/coverage/shingles-
shots
32. French MT, Homer J, Gumus G, and Hickling L. Key Provisions of the Patient Protection and Affordable
Care Act (ACA): A Systematic Review and Presentation of Early Research Findings. Health Serv Res.
2016 Oct; 51(5): 1735-1771.
33. Courtemanche C, Marton J, et al. The three‐year impact of the Affordable Care Act on disparities in
insurance coverage. Health Serv Res. 2019 Feb; 54(Suppl 1): 307–316.
34. Glied S, Ma S, and A Borja. Commonwealth Issue Brief: Effect of the Affordable Care Act on Health Care
Access. May 2017. https://www.commonwealthfund.org/
35. Centers for Disease Control and Prevention. Health, United States, 2019.
https://www.cdc.gov/nchs/data/hus/hus19-508.pdf
36. Agency for Healthcare Research and Quality. 2019 National Healthcare Quality and Disparities Report.
https://www.ahrq.gov/research/findings/nhqrdr/
37. Borsky A, Zhan C, Miller T, et al. Few Americans Receive All High-Priority, Appropriate Clinical
Preventive Services. Health Affairs, 37(6):925-928. doi: 10.1377/hlthaff.2017.1248.
38. Alharbi A, Khan MM, Horner R, et al. Impact of removing cost sharing under the Affordable Care Act
(ACA) on mammography and pap test use. BMC Public Health. 2019; 19(1): 370.
39. Huguet N, Angier H, Rdesinski R, et al. Cervical and colorectal cancer screening prevalence before and
after Affordable Care Act Medicaid expansion. Preventive Medicine, Volume 124 (July 2019):91-97.
40. Li Y, Toseef MU, Jensen GA, et al. Gains in insurance coverage following the affordable care act and
change in preventive services use among non-elderly US immigrants. Preventive Medicine, 148(2021):
106546.

JANUARY 2022
ISSUE BRIEF
13
41. Agency for Healthcare Research and Quality. Achieving Health Equity in Preventive Services:
Systematic Review. December 2019. https://effectivehealthcare.ahrq.gov/products/health-equity-
preventive/research
42. Lee LK, Chien A, Stewart A, et al. Women’s Coverage, Utilization, Affordability, And Health After The
ACA: A Review of the Literature. Health Affairs, May 2020; 39(3).
43. Fletcher G, Alatevi EM, Genao A, et al. Disparities in Colorectal Cancer Screening: The Effect of ACA
Medicaid Expansion on Minorities and Low-Income Populations. Gastroenterology, Volume 156(6),
Supplement 1, May 2019:S-183.
44. U.S. Preventive Services Task Force. Final Recommendation Statement: Colorectal Cancer Screening.
uspreventiveservicestaskforce.org
45. ASPE analysis of 2019 American Community Survey Public Use Microdata Sample (ACS PUMS)
46. Bhandari NR and Li C. 2018. Impact of the Affordable Care Act (ACA)’s Elimination of Cost-Sharing
Provision on the Guideline-Recommended Cancer Preventive Screenings in the United States. Value in
Health, Volume 21, Supplement 1: S131-S132. https://doi.org/10.1016/j.jval.2018.04.881
47. Annual Report to the Nation on the Status of Cancer, Part 1: National Cancer Statistics. JNCI: Journal of
the National Cancer Institute. Oxford Academic. oup.com
48. Pisu M, Henrikson NB, Banegas MP, and R Yabroff. Costs of Cancer Along the Care Continuum: What
We Can Expect Based on Recent Literature. Cancer (2018); 124:4181-4191.
49. Leopold C, Park E, Nekhlyudov L. The Impact of the Affordable Care Act on Cancer Survivorship. The
Cancer Journal, May/June 2017, Volume 23(3):181-189.
50. Chu QD, Li T, Hsieh M, et al. Positive Impact of the Patient Protection and Affordable Care Act
Medicaid Expansion on Louisiana Women with Breast Cancer. Cancer, March 2021, Volume
127(5):688-699.
51. Cancino RS, Su Z, et al. The Impact of COVID-19 on Cancer Screening: Challenges and Opportunities.
JMIR Cancer. 2020 Jul-Dec; 6(2): e21697.
52. London JW, Fazio-Eynullayeva E, Palchuk MB, et al. Effects of the COVID-19 pandemic on cancer-
related patient encounters. JCO Clinical Cancer Informatics. 2020(4) July: 657-665.
53. Lipton, B and Becker, S. ACA Provisions Associated with Increase in Percentage of Young Adult Women
Initiating and Completing The HPV Vaccine. Health Affairs, May 2015.
54. Hawkins SS, Horvath K, et al. Associations between insurance-related affordable care act policy
changes with HPV vaccine completion. BMC Public Health, 2021; 21: 304.
55. Han, X, Yabroff R, et al. Has recommended preventive service use increased after elimination of cost-
sharing as part of the Affordable Care Act in the United States. Preventive Medicine, Volume
78(September 2015):85-91.
56. Hung MC, Williams WW, Lu PJ, Kim DK, Grohskopf LA, Pilishvili T, et al. Vaccination Coverage Among
Adults in the United States. National Health Interview Survey, 2016.
https://www.cdc.gov/vaccines/imz-managers/coverage/adultvaxview/pubs-resources/NHIS-2016.html
57. Aris E, Montourcy M, et al. The adult vaccination landscape in the United States during the Affordable
Care Act era: Results from a large retrospective database analysis. Vaccine, Volume 38, Issue 14
(March 23, 2020): 2984-2994.
58. Lind K, Hildreth KL, Perraillon MC. Persistent Disparities in Medicare's Annual Wellness Visit Utilization.
Medical Care, December 2019, Volume 57(12):984-989.
59. Ruhl C. Contraception is Health Promotion. Nursing for Women's Health, Volume 16(1):73-77
60. Fletcher JM, Wolfe BL. Education and Labor Market Consequences of Teenage Childbearing. Journal of
Human Resources, 44(2):303-325.
61. Bailey MJ. Fifty years of family planning: new evidence on the long-run effects of increasing access to
contraception [Internet]. Cambridge (MA): National Bureau of Economic Research; 2013 Oct [cited
2015 May 15]. (NBER Working Paper No. 19493). http://www.nber.org/papers/w19493.pdf

JANUARY 2022
ISSUE BRIEF
14
62. Dalton VK, Carlos RC, Kolenic GE, Moniz MH, Tilea A, Kobernik EK, and Fendrick AM. 2018. The impact
of cost sharing on women’s use of annual examinations and effective contraception. American journal
of obstetrics and gynecology, 219(1), 93-e1.
63. Pace LE, Dusetzina SB, Fendrick AM, Keating NL, and Dalton VK. 2013. The impact of out-of-pocket
costs on use of intrauterine contraception among women with employer-sponsored insurance.
Medical Care, 51(11), 959.
64. Pace LE, Dusetzina SB, and Keating NL. 2016. Early impact of the Affordable Care Act on oral
contraceptive cost sharing, discontinuation, and nonadherence. Health Affairs, 35(9), 1616-1624.
65. Trussell J, Lalla AM, Doan QV, Reyes E, Pinto L, Gricar J. Cost effectiveness of contraceptives in the
United States. Contraception. 2009 Jan;79(1):5-14. doi: 10.1016/j.contraception.2008.08.003. Epub
2008 Sep 25. Erratum in: Contraception. 2009 Aug;80(2):229-30. PMID: 19041435; PMCID:
PMC3638200.
66. Becker N and Polsky D. 2015. Women Saw Large Decrease in Out-of-Pocket Spending for
Contraceptives after ACA Mandate Removed Cost Sharing. Health Affairs, 34(7), 1204-1211.
67. Carlin CS, Fertig AR and Down BE. Affordable Care Act’s mandate eliminating contraceptive cost-
sharing influenced choices of women with employer coverage, Health Affairs, 2016, 35(9):1608–1615.
68. Becker NV, Keating NL, and Pace LE. 2021. ACA Mandate Led To Substantial Increase In Contraceptive
Use Among Women Enrolled In High-Deductible Health Plans: Study examines contraceptive use
among women enrolled in high-deductible health plans, comparing before and after an ACA
contraceptive coverage mandate. Health Affairs, 40(4), 579-586.
69. Myerson R, Crawford S, and Wherry LR. Medicaid Expansion Increased Preconception Health
Counseling, Folic Acid Intake, And Postpartum Contraception. Health Affairs, 2020, 39(11): 1883-1890.
70. Geiger CK, Sommers BD, Hawkins SS, and Cohen JL. Medicaid expansions, preconception insurance,
and unintended pregnancy among new parents. Health Services Research, 2021;56:691-701.
https://doi.org/10.1111/1475-6773.13662
71. National Center for Health Statistics. Key Statistics from the National Survey of Family Growth:
Intendedness of pregnancy. https://www.cdc.gov/nchs/nsfg/keystatistics.htm
72. Sommers B, Maylone B, Blendon RJ, et al. Three-Year Impacts of the Affordable Care Act: Improved
Medical Care and Health among Low-Income Adults. Health Affairs, June 2017, Volume 36(6):1119-28.
https://www.healthaffairs.org/doi/10.1377/hlthaff.2017.0293
73. Dai H and AS Khan. The Effects of the Affordable Care Act on Health Access among Adults Aged 18-64
Years with Chronic Health Conditions in the United States, 2011-2017. Journal of Public Health
Management and Practice, September 9, 2020.
74. Ward BW. Barriers to Health Care for Adults with Multiple Chronic Conditions: United States, 2012–
2015. NCHS Data Brief No. 275, March 2017.
75. Han, X, Yabroff R, et al. Has recommended preventive service use increased after elimination of cost-
sharing as part of the Affordable Care Act in the United States. Preventive Medicine, Volume
78(September 2015):85-91.
76. Cole MB, Kim J, and TW Levengood. Association of Medicaid Expansion With 5-Year Changes in
Hypertension and Diabetes Outcomes at Federally Qualified Health Centers. JAMA Health Forum.
2021;2(9):e212375. doi:10.1001/jamahealthforum.2021.2375
77. Soni A, Wherry LR, and KI Simon. How Have ACA Insurance Expansions Affected Health Outcomes?
Findings from the Literature. Health Affairs, 39(3): 371-378.
78. Ginossar T, Van Meter L, et al. Early Impact of the Patient Protection and Affordable Care Act on
People Living With HIV: A Systematic Review. Journal of the Association of Nurses in AIDS Care. May-
June 2019, Volume 30(3):259-269.
79. ASPE. Trends in the U.S. Uninsured Population, 2010-2020. https://aspe.hhs.gov/pdf-report/us-
uninsured-population-trends
80. ASPE. Health Insurance Coverage and Access to Care Among Latinos: Recent Trends and Key
Challenges. https://aspe.hhs.gov/reports/health-insurance-coverage-access-care-among-latinos

JANUARY 2022
ISSUE BRIEF
15
81. ASPE. Health Insurance Coverage and Access to Care for American Indians and Alaska Natives: Current
Trends and Key Challenges. https://aspe.hhs.gov/reports/health-insurance-coverage-changes-aian
82. ASPE. Health Insurance Coverage Among Working-Age Adults with Disabilities: 2010-2018.
https://aspe.hhs.gov/reports/health-insurance-coverage-among-working-age-adults-disabilities-2010-
2018

JANUARY 2022
ISSUE BRIEF
16
U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES
Office of the Assistant Secretary for Planning and Evaluation
200 Independence Avenue SW, Mailstop 447D
Washington, D.C. 20201
For more ASPE briefs and other publications, visit:
aspe.hhs.gov/reports
SUGGESTED CITATION
Access to Preventive Services without Cost-sharing:
Evidence from the Affordable Care Act (Issue Brief No. HP-2022-
01). Office of the Assistant Secretary for Planning and Evaluation,
U.S. Department of Health and Human Services. January 2022.
COPYRIGHT INFORMATION
All material appearing in this report is in the public domain and
may be reproduced or copied without permission; citation as to
source, however, is appreciated.
DISCLOSURE
This communication was printed, published, or produced and
disseminated at U.S. taxpayer expense.
___________________________________
Subscribe to ASPE mailing list to receive
email updates on new publications:
https://list.nih.gov/cgi-bin/wa.exe?SUBED1=ASPE-HEALTH-POLICY&A=1
For general questions or general
information about ASPE:
aspe.hhs.gov/about
HP-2022-01
