This PDF is a selection from an out-of-print volume from the National Bureau
of Economic Research
Volume Title: Advances in the Economics of Aging
Volume Author/Editor: David A. Wise, editor
Volume Publisher: University of Chicago Press
Volume ISBN: 0-226-90302-8
Volume URL: http://www.nber.org/books/wise96-1
Conference Date: May 6-9, 1993
Publication Date: January 1996
Chapter Title: Health Insurance and Early Retirement: Evidence from the
Availability of Continuation Coverage
Chapter Author: Jonathan Gruber, Brigitte C. Madrian
Chapter URL: http://www.nber.org/chapters/c7320
Chapter pages in book: (p. 115 - 146)

4
Health Insurance and Early
Retirement: Evidence from the
Availability of Continuation
Coverage
Jonathan Gruber and Brigitte
C.
Madrian
The dramatic postwar decline in the labor force participation of older men in
the United States has motivated a sizable body of literature on retirement be-
havior. Three factors, in particular, have been studied extensively: the growth
of the Social Security program (see, for example, Burtless 1986; Burtless
and Moffitt 1984; Diamond and Hausman 1984; Hausman and Wise 1985;
Sueyoshi 1989), the increased availability and generosity
of
private pensions
(Stock and Wise 1990a, 1990b), and the expansion of federal disability insur-
ance (Bound and Waidmann 1992). One potentially important factor that until
recently has not received much attention is the availability of health insurance
for retirees. This oversight is especially surprising given the rather consistent
evidence that health status is an important determinant in the retirement deci-
sion (Bazzoli 1985; Diamond and Hausman 1984). If health status matters in
the decision about when to retire, it seems quite natural that health insurance
should matter as well.
The increased availability
of
health insurance for older Americans, espe-
cially retirees, has come in several forms. First among them is the introduction
in the mid- 1960s of Medicare, a federal program that provides near-universal
health insurance coverage for those over age 65. A second source of health
insurance that has grown in importance, particularly for those under age 65
who are not yet eligible for Medicare, is employer-provided postretirement
health insurance. While only
30%
of men who retired in the early 1960s re-
Jonathan Gruber is associate professor of economics at the Massachusetts Institute of Technol-
ogy and a faculty research fellow of the National Bureau of Economic Research. Brigitte C. Ma-
drian is assistant professor of economics at the University of Chicago and a faculty research fellow
of the National Bureau of Economic Research.
The authors wish to thank David Cutler, James Poterba, Andrew Samwick, Richard Zeckhauser,
and seminar participants at
Hanard,
MlT,
and the NBER for their comments, and Aaron Yelowitz
for his help
in
assembling the
SIPP
data.
They also acknowledge financial support from the James
Phillips Fund, the
Harry
and Lynde Bradley Foundation, and the National Institute on Aging.
115

116
Jonathan
Gruber
and Brigitte
C.
Madrian
ceived health insurance from their former employers,
this
fraction increased to
almost half for those retiring in the 1980s (Madrian 1994).
This paper looks at the effect on retirement of a third source of health insur-
ance for early retirees, namely continuation coverage benefits. During the late
1970s and early 1980s many states mandated that employers allow employees
who leave their jobs to continue purchasing their group health insurance for a
specified number of months. These continuation benefits were extended to all
workers in 1986 as part of the federal Consolidated Omnibus Budget Reconcil-
iation Act (COBRA) legislation. Although this coverage is available to all
workers regardless of age, it should be particularly attractive to older workers
who face a relatively high price for health insurance in the private market and
who are more likely to be subject to the preexisting-conditions exclusions that
are characteristic of such policies.
To
identify the effect of continuation benefits on retirement, we exploit the
fact that these benefits were mandated at different times by different states
(and finally the federal government) and that the generosity of the mandates
varied across states as well. Using data from the Current Population Survey
(CPS), we find a strong correlation between the availability of continuation
benefits and the likelihood that individuals are retired. Our key finding is that,
among men aged
55-64,
one year of continuation benefits increases the proba-
bility
of
being retired by
1
percentage point; this is
5.4%
of the baseline proba-
bility of being retired for
this
group. Furthermore, we find that, although the
estimated percentage-point effects are strongest near the age of Medicare eligi-
bility, as a fraction of baseline retirement probabilities they actually decline
with age. Although this latter result is somewhat counterintuitive, it is consis-
tent with other work that examines the effect of continuation coverage on flows
into retirement (Gruber and Madrian 1995). We also find that continuation
coverage mandates significantly increase the likelihood that early retirees are
covered by employer-provided health insurance after retirement. This effect is
much larger than the implied effect on retirement, suggesting that much of the
increase in coverage is occumng among those individuals who would have
retired even in the absence of such benefits.
The organization of the paper is as follows. Section 4.1 provides some moti-
vation for why health insurance should matter in the early retirement decision.
Section 4.2 outlines the state and federal continuation coverage laws, which
we use to identify the effect of health insurance on retirement. This is followed
in section
4.3
by a model that formalizes the effect of health insurance
on
retirement. The data and regression framework are presented in section 4.4,
and the results follow in section 4.5 along with a comparison with our findings
from dynamic models of retirement behavior. Section 4.6 considers the impact
of continuation coverage mandates on insurance coverage. The paper con-
cludes in section 4.7 with a discussion of the methodological and policy impli-
cations of our results.

117
Health Insurance and Retirement
4.1
Health Insurance and Retirement: Should It Matter?
The high and variable level of medical expenditures for persons aged 55-64,
without the guarantee of public coverage through Medicare for those over age
65,
means that the availability of health insurance coverage could be a key
factor in determining the timing of retirement. Until recently, however, there
has been little study of the effect of retiree health insurance coverage
on
retire-
ment patterns. Two recent papers have attempted to model the role of health
insurance
in
the retirement decision. Lumsdaine, Stock, and Wise (1994) in-
corporate the value of Medicare into an option value model of retirement and
find
no
effect of Medicare eligibility
on
the retirement hazard. Their result is
not surprising, however, as they estimate their model
on
a sample of workers
from the same firm, all of whom have employer-provided postretirement health
insurance that is much more generous than Medicare. Gustman and Steinmeier
(1994) use information from the Retirement History Survey, a longitudinal sur-
vey from the 1970s, to ascertain whether individuals have employer-provided
retiree health insurance, and data from the 1977 National Medical Care Expen-
diture Survey, to impute the value of that insurance based
on
individual charac-
teristics. They also find very small effects of retiree health insurance
on
retire-
ment decisions.
The results of these two studies are at odds with
both
intuition and with what
individuals report about the importance of health insurance in the retirement
decision.
In
a recent Gallup poll, 63% of working Americans reported that they
“would delay retirement until becoming eligible for Medicare [age 651 if their
employers were not going to provide health coverage” despite the fact that
50%
“said they would prefer to retire early-by age 62” (Employee Benefits
Research Institute 1990). The apparent contradiction between the importance
of health insurance as stated by individuals and that estimated by these two
previous studies provides a further motivation for our research.
4.1.1
Health Status of Older Individuals
That individuals should cite health insurance as an important consideration
in the retirement decision is not surprising, as older persons are fairly likely
to need expensive medical care. Tables 4.1-4.4 compare the health status of
individuals by age along a number of dimensions. The simplest measure, self-
reported health status, is shown in table 4.1. The fraction of individuals who
report being in fair
or poor
health increases markedly from ages
45-54
(19.7%) to ages 55-64 (31.3%). While recent research has suggested that self-
reported health status may be a poor indicator of the actual severity of an indi-
vidual’s clinical conditions (Bazzoli 1985), it may be the most accurate mea-
sure of an individual’s valuation of health insurance coverage. Thus, these fig-
ures suggest that insurance valuation will rise dramatically with age.
Furthermore, as table 4.2 shows, health status as measured by doctor-

118
Jonathan
Gruber
and Brigitte
C.
Madrian
Table
4.1
Self-Reported Health
Status
by Age
(%)
Health Status
Age Excellent
Good
Fair
Poor
25-34 36.4 53.1
9.5
1.1
35-44 32.0
54.6
11.9 1.5
45-54 27.8
52.5 15.6 4.1
55-64
18.0 50.7
24.9 6.4
65
+
9.3 43.1
36.1 11.4
Source:
Authors’ calculations using data from the
1987
National Medical Expenditure Survey.
Note:
The numbers in the table give the fraction
of
individuals who report having the given
health status.
Table
4.2
Incidence of Health Problems by Age
(%)
Condition
25-34 35-44 45-54 55-64 65
+
Stroke
Cancer
Heart attack
Gallbladder disease
High blood pressure
Arteriosclerosis
Rheumatism
Emphysema
Arthritis
Diabetes
Heart disease
Any
of
the above
0.4
1.6
0.3
1.6
10.1
0.2
0.8
0.4
5.1
1.7
0.8
18.2
0.8
2.4
1.1
3.6
18.2
0.6
1.6
1
.o
11.6
3.0
2.2
31.7
1.6
4.7
3.8
7.3
29.1
2.8
5.2
2.6
24.9
5.7
6.1
51.8
3.6
9.7
7.7
9.4
41.9
6.1
8.2
5.2
41.2
9.8
11.9
72.3
7.4
13.3
13.3
14.6
49.8
16.3
16.4
8.0
54.9
14.7
22.2
84.2
Source:
Authors’ calculations using data from the
1987
National Medical Expenditure Survey.
Nure:
The numbers in the table give the fraction
of
individuals who report ever having had the
listed medical condition.
diagnosed health problems deteriorates with age as well. The incidence
of
many
of
the health problems listed (stroke, cancer, heart attack, arteriosclero-
sis, emphysema, and heart disease) more than doubles between
45-54
and ages
55-64.
Furthermore, almost three-quarters
of
those aged
55-64
have been di-
agnosed with at least one
of
the eleven conditions listed. Not surprisingly, rela-
tive to those aged
45-54,
individuals
55-64
are more likely to be admitted to
the hospital over the course
of
a year and spend more time there once admitted
(table
4.3).
The most direct evidence that health insurance should be valued relatively
highly by older workers, however, is that the actual medical expenses incurred
by those aged
55-64
are much higher than those
of
younger individuals (table
4.4).
In every category not only do expenditures rise with age, but the variance

119
Health Insurance and Retirement
Table
4.3
Annual Medical Care Utilization by Age
25-34 35-44 45-54 55-64 65+
Fraction admitted to hospital
(%)
9.2 6.8 8.7
11.0
20.1
Number of admissions (if ever
Nights in hospital (if ever
admitted)
1.17 1.24 1.39 1.5
1.5
admitted)
5.5
6.8 9.3 11.8 13.8
(%)
52.9 55.6 61.1 71.1 81.9
(if any prescribed medicines)
5.2 6.6 11.5 14.7
18.5
Fraction
who
visited a doctor
(%)
64.1 67.1 71.1 77.9
85.8
visited a doctor)
4.6 4.6 5.5 6.0 7.4
Fraction with prescribed medicines
Number of prescribed medicines
Number of doctor visits (if
Source:
Authors’ calculations using data from the
1987
National Medical Expenditure Survey.
Table
4.4
Average Annual Medical Expenditures by Age
(1990
dollars)
25-34 35-44 45-54 55-64 65-74 75+
Average expenditures
Hospitdinpatient
Physiciadoutpatient
Prescription medication
Total
Average expenditure if
HospitaYinpatient
Physicidoutpatient
Prescription medication
expenditure
>
0
Total
Source:
Authors’ calculations using
data
from the
1980
National Medical Care Utilization and
Expenditure Survey (inflated to
1990
dollars using the Medical Care Component of the consumer
price index).
Note:
Standard deviation
of
expenditures is in parentheses.

120
Jonathan
Gruber
and Brigitte
C.
Madrian
increases as well.
In
1990
dollars, total medical expenditures of those 55-64
averaged
$2,144.
This
represents 5.4% of average total family income for this
age group, 6.9% of average total family income for retired individuals, and
30%
of the average pension income of early retirees.'
A
one-standard-deviation
increase in expenditures for a 55-64-year-old would represent an additional
16.5% of family income. Total
family
medical expenditures would naturally
constitute a much higher fraction of income. Thus, it is easy to see why older
individuals should be concerned about their health insurance coverage after
retirement.
4.1.2 Health Insurance Coverage and Costs
Given the costs of health care for older workers, it should not be surprising
that older individuals are no more likely to be uninsured than their younger
counterparts, as is shown in table 4.5. The sources of health insurance cover-
age, however, differ with age. Even though employment-based health insur-
ance is the predominant source of coverage regardless of age, older individuals
are less likely than younger persons to have employment-based health insur-
ance and much more likely to be covered by a nongroup (individual) or other
group policy. This suggests that individuals who retire early but who do not
have access to employer-provided health insurance turn to the individual mar-
ket for insurance.
The bottom two panels of table 4.5 break down the sources of health insur-
ance coverage by employment status. There are three major differences be-
tween the sources of health insurance coverage for those who are and are not
employed. First, one-fifth of nonworking older persons are insured through
Medicare or Medicaid, while only
1
%
of the older employed receive coverage
from one of these two sources. Second, older nonworking individuals are 40%
less likely to be uninsured than their younger counterparts. Third, relative to
the young, the older nonworking are six times more likely to be covered by
employer-provided health insurance in their own name.
These last two differences are explained in large part by the availability of
employer-provided postretirement health insurance. Forty-five percent of indi-
viduals work in firms that provide retiree health insurance benefits.* The older
nonworking, who are more likely to be retired than the young nonworking, are
therefore more likely to be covered by employer-provided retiree health in-
surance.
There are, nevertheless, a substantial number of older individuals who are
not covered by either employer or government-provided health insurance. It is
these individuals who find themselves in the market for individual health insur-
ance and who we would therefore expect to benefit from the availability of
1.
Exoenditures as a fraction of income are calculated using income data from the March
1990
-
CPS
.
2.
See Madrian
(1994)
for background
on
the structure
and
availability of postretirement
health insurance.

121
Health Insurance and Retirement
Table
4.5
Insurance Coverage by Age
and
Employment Status
(%)
Employment-
Based
Other CHAMPUS/ Medicare/
Any Own Name Group Nongroup CHAMPVA Medicaid Uninsured
~~~~
All individuals
25-54 71.6 51.1 1.2 5.9 5.7 5.6 15.4
55-64 64.5 44.8 4.1 14.5 7.7 10.4 12.0
25-54 78.5 62.7
1.1
5.8 4.9 1.2 13.5
55-64 76.3 63.1 4.0 12.6 6.8 0.8 10.1
25-54 44.2 4.2 1.3 6.2 8.8 23.4 23.0
55-64 51.6 24.7 4.3 16.6 9.2 20.9 14.1
Source:
Authors’ calculations using data from the
1987
National Medical Expenditure Survey.
Employed
Not employed
continuation coverage. The reason is simple-insurance in the individual mar-
ket is typically quite expensive.
Employers have significant cost advantages in providing health insurance.
By pooling the risks of many individuals, they are able to lower administrative
expenses and reduce adverse selection. These two factors alone are estimated
to reduce the cost
of
providing insurance in large (ten thousand or more em-
ployees) firms relative to small (one to four employees) firms by 40%
(Con-
gressional Research Service 1988). For older individuals the cost differential
between employer-provided and individual health insurance is exacerbated be-
cause policies in the individual market are typically age-rated, while within
the
firm
younger workers subsidize the health insurance costs of their older
coworkers. The Congressional Research Service (1988) reports that the cost to
employers of providing insurance coverage for 55-64-year-old males is three
times that of providing coverage to males under 40; for females, the ratio is
two to 0ne.3
In Massachusetts the average cost of family health insurance coverage per
employee in 1989 was $3,882.4 When inflated by the medical care component
of the consumer price index, this is equivalent to
$5,047
in 1993 dollars.
In
contrast, a New England commercial insurance company is offering a family
policy for a 58-year-old male with
a
one-year preexisting-conditions exclusion
at a price of $8,640. This represents 26% of the average family income of
retired individuals aged 55-64 in Massachusetts. Individual policies may also
be medically underwritten
so
that sick individuals may face substantially
higher prices or may not be able to purchase a policy at all.
3.
Of course, to the extent employer costs can be shifted to the wages of employees in
an
age-
4.
Authors’ calculation using unpublished data from the Health Insurance Association
of
specific fashion, older individuals will bear these higher costs. See the discussion in section
4.3.
America.

122
Jonathan
Gruber
and
Brigitte C.
Madrian
The coverage available in the private market not only is expensive, but also
is typically less generous than employer-provided health insurance. Table
4.6
compares the health insurance benefits of individuals covered under group and
nongroup policies in
1977.
In every category, those covered under nongroup
policies receive more limited benefits. Relative to those with nongroup cover-
age, those with group policies are more than twice as likely to receive major
medical coverage or coverage for physician office visits and prescription drugs,
and more than
50%
more likely to receive ambulance, mental health, and out-
patient diagnostic service coverage. Furthermore, nongroup policies generally
feature both higher deductibles and higher copayments. Thus, relative to the
individual market, group coverage offers individuals higher-quality insurance
coverage at a significantly lower price.
4.2
Continuation Coverage Laws
For those individuals whose employers do not offer retiree health insurance,
an alternative to purchasing health insurance in the individual market is pro-
vided by various state and federal continuation coverage laws. These laws man-
date that employers sponsoring group health insurance plans offer terminating
employees and their families the right to continue their health insurance cover-
age through the employer’s plan for a specified period of time. The laws gener-
Table
4.6
Group
and
Nongroup Health
Insurance
Benefits,
1977
(%)
Fraction
of
Individuals
with
Specified Benefit
Group Plans Nongroup Plans
Primary benefits
Major medical coverage
86.9 39.1
Hospital room and board 98.4 91.4
Surgery
97.6 91.6
Physician office visit
87.9 40.4
Ambulance
89.0 54.0
Outpatient diagnostic services 95.9 66.0
hescribed medicines
87.3 30.3
Mental health
92.2 66.0
Other benefits
Generosity
of
benefits (conditional on
having benefit)
Major medical deductible
<
$100 94.3 61.6
Full semiprivate room charge 77.8 38.2
80-100%
of
usual common
and
reasonable surgical charge 70.6 60.0
80-100%
of
usual common
and
reasonable physician charge 91.8 81.3
Source:
Farley (1986), tables
45-58.

123
Health Insurance and Retirement
ally apply to all separations (except those due to an employee’s gross miscon-
duct), although in some states benefits are restricted to those who leave their
jobs in~oluntarily.~ They often also provide benefits to divorced or widowed
spouses and their families. The first such law was implemented by Minnesota
in 1974. More than twenty states passed similar laws over the next decade
before the federal government, as part of the 1985 COBRA, mandated such
coverage at the national level. Continuation coverage is now commonly re-
ferred to as COBRA coverage, a nomenclature we will also use.
The various state statutes are summarized in table 4.7.6 The length of cover-
age is generally quite short, from three to six months, although nine states
mandate coverage of nine months or more. Although most state laws stipulate
that an employee must have been covered by an employer’s insurance for three
to six months before being eligible for continuation coverage, this requirement
is not likely to be binding on older workers, most of whom have been with
their current employer for many years.’ The state laws also apply only to firms
that actually purchase insurance through an insurance company; self-insured
firms, under the 1974 Employee Retirement Income and Security Act
(ERISA), are not subject to these (or any other) state mandates.*
Although similar in spirit, the state and federal laws differ in a number of
important ways. First, the length of coverage mandated under the federal law,
eighteen months, equals or exceeds that mandated by all but one state (as of
January 1987, Connecticut law provides for up to twenty months of c~verage).~
Second, there is no minimal length of time for which an employee must be
covered under an employer’s plan before being eligible for continuation bene-
fits. Third, the federal law applies to self-insured firms, who are exempt from
the state laws, as well as to those who purchase their coverage from insurers.
The federal law, however, does not apply to small firms employing less than
twenty workers. Finally, employees of religious organizations and the federal
government were exempt from COBRA, although federal employees have sub-
sequently been included (beginning in 1990). When the specific details of the
5. Because retirement is a voluntary separation, we treat those states whose laws apply only to
involuntarily terminated employees as states without laws.
6.
Details on state laws are from Hewitt (1985) and Thompson Publishing Group (1992) and
have been cross-checked against the actual state statutes. Table
4.7
lists only those states with laws
that apply to employees who terminate their employment voluntarily.
7.
Almost 95%
of
retirees have job tenure of at least ten years by the time they retire (Madrian
1994).
8.
In a related paper we incorporate a correction factor that accounts for the exclusion of some
firms
from the effects of these laws
(Gruber
and Madrian 1995). This has little effect on the sig-
nificance of the estimates
of
the effect of continuation coverage on retirement, although the magni-
tude increases two- to threefold.
9. Eighteen months is the maximum length of coverage available following the voluntary
or
involuntary termination of employment. COBRA
also
provides up to thirty-six months of coverage
for family members who would otherwise lose their insurance coverage through events such as an
employee’s death, divorce
from the employee,
or
the employee’s eligibility for Medicare.

124
Jonathan
Gruber
and Brigitte
C.
Madrian
Table
4.7
State
Continuation Coverage
Laws
Effective Months of Effective Months
of
State Date Coverage State Date Coverage
Arkansas
California
Colorado
Connecticut
Georgia
Illinois
Iowa
Kansas
Kentucky
Minnesota
Missouri
Nevada
New Hampshire
New Mexico
7/20/79
1/1/85
7/1/86
10/1/75
1/1/87
7/1/86
1/1/84
8/23/85
7/1/87
1/1/78
7/15/80
81 1 174
3/19/83
6/1/87
9/28/85
1/1/88
8/22/8 1
7/1/83
4
3
3
10
20
3
6
9
9
6
9
6
12
18
9
18
10
6
New
York
North Carolina
North Dakota
Oklahoma
Oregon
mode Island
South Carolina
South Dakota
Tennessee
Texas
Utah
Vermont
Virginia
Wisconsin
1/1/86
1/1/82
7/1/83
1/1/76
1/1/82
1/1/88
1/1/79
1/1/90
7/1/84
3/3/88
1/1/81
1/1/81
7/1/86
5/14/86
4/17/86
5/14/80
6
3
10
1
6
18
2
6
3
18
3
6
2
6
3
18
Sources:
Hewitt
(1985);
Thompson F’ublishing Group
(1992);
state statutes.
state and federal statutes are at odds, firm provision of continuation benefits is
governed by the law that provides for more generous coverage.
The effective dates of the state laws are listed in table 4.7. The federal cover-
age mandated under COBRA was phased in. Beginning in July 1986, firms
had to offer continuation benefits at the
start
of their next plan year. For work-
ers provided health insurance under union contracts, such benefits did not have
to be offered until the next contract negotiation after January 1987.
Both the state and federal laws stipulate that the employee must pay the full
cost of the coverage. At the federal level,
this
is defined specifically as 102%
of the average employer cost of providing coverage. The coverage must be
identical
to
that provided to similarly situated active employees, including the
option to continue enrollment in supplemental insurance plans (such as for
vision or dental care) if these are available. Although 102%
of
the employer’s
cost is typically much more than individuals pay as active employees, it
is,
as
already noted, substantially less than the cost of buying equivalent coverage in
the private market, especially for older workers.
Because continuation coverage is a relatively new phenomenon (at least at
the national level), information on the extent of continuation coverage is some-
what scarce. Zedlewski (1993) estimates that, in 1988,5.2% of retired workers
aged 55-64 were covered by COBRA health insurance. This figure must be
interpreted relative to the number of individuals who could be expected to
take up such coverage. The 52% of individuals aged 55-64 with retiree health
insurance are not likely to be covered, and the 21% of individuals who were

125
Health Insurance and Retirement
not insured through their former employer are not eligible. Similarly, those
who have been retired for more than eighteen months have exceeded their po-
tential eligibility. Tabulations from the 1987 National Medical Expenditure
Survey indicate that one-third of retired individuals aged
55-64
have been re-
tired for less than eighteen months. If we take the group who could potentially
be affected by COBRA to be one-third of retired individuals between ages
55
and
64
who worked in firms that provided health insurance but did not provide
retiree health insurance, we would expect at most 9% of early retirees to be
covered. That 5.2% receive continuation benefits suggests that
58%
of
the re-
tired population who would be at all likely to be covered by COBRA actually
are. As knowledge about the availability of such coverage has become more
widespread since 1988, this fraction may be higher today.
An alternative calculation is possible using figures reported in Flynn (1992).
She uses data from a large firm that administers COBRA claims to estimate
that 23% of individuals who qualified for COBRA coverage because of retire-
ment elected to receive benefits. If we expected only the
30%
of individuals in
firms that offer health insurance but do not offer retiree health insurance to
even consider purchasing COBRA insurance,
this
take-up rate implies that
75%
of those most likely to be covered by continuation benefits actually are.
Both of these calculations, therefore, suggest that retirees without an altema-
tive source of health insurance coverage are quite likely to elect continuation
coverage.
For all COBRA beneficiaries, the average length of time
on
COBRA was
seven months (Flynn 1992). Individuals over age
61,
however, maintained their
coverage for a much longer period of time-about twelve months on average.
This finding is not surprising for two reasons. First, younger individuals are
more likely to find alternative coverage through a new job or a spouse’s em-
ployment. Second, COBRA coverage provides a larger subsidy for older work-
ers; with a lower relative price, they should therefore demand more coverage.
Table 4.8 compares the distribution of health insurance coverage in 1984,
two years before COBRA was first implemented, and in 1989, two years after
it had been phased in. Note that employment-based health insurance coverage
is
more prevalent after COBRA, and that
this
effect is confined to those who
are not employed, exactly
the
group whom we would expect to be insured
under COBRA.
This
finding is similar to evidence presented in Rogowski and
Karoly (1 992), who examined the primary source of insurance coverage after
retirement, based
on
the source of insurance coverage before retirement, before
and after COBRA. They find that in the pre-COBRA period,
72%
of individu-
als who retired from jobs with employment-based health insurance continued
to be covered by that insurance upon retirement. After COBRA, this figure
rises to
78.5%.1°
Taken together,
the
evidence
on
take-up rates and the increase
in the extent of employer-provided health insurance coverage among early re-
10.
We
present a stronger test of the effect
of
continuation coverage mandates on insurance
coverage in section
4.6.

126
Jonathan
Gruber
and
Brigitte
C.
Madrian
Table
4.8
Health Insurance Coverage before
and
after
COBRA
(%)
-
~~~~ ~ ~~
All Individuals Employed Not Employed
25-54 55-64 25-54 55-64 25-54 55-64
Insurance coverage in
1984
Any private health insurance
Health insurance in own name
Employ ment-based
Not employment-based
Covered as a dependent
Insurance coverage in
1989
Any private health insurance
Health insurance in own name
Employment-based
Not employment-based
Covered as a dependent
82.1 83.7 89.1 92.5 60.1 74.1
52.1 47.4 66.7
68.9
5.9 23.6
5.1 12.5
5.1
10.4 5.2
14.7
24.2 23.4 16.8
12.8 47.7
35.0
82.4 84.3 88.6 92.1 57.3 74.9
54.7
49.2 66.4
68.1 7.1 26.6
5.3
12.9
5.2
9.6
5.2 16.8
22.0 21.8
16.4
14.4 43.7
30.6
Source:
Authors' calculations using data
from
the Survey
of
Income and Program Participation,
1984
Wave
3
and
1987
Wave
7.
tirees after COBRA suggests that older workers who retire early and who
do
not have an alternative source of coverage actually avail themselves of the con-
tinuation benefits to which they are entitled.
4.3
Modeling the Effect
of
Health Insurance on Retirement
We present a simple graphical exposition of the effect of health insurance
benefits on the retirement decision, along the lines of Burtless (1986) and Burt-
less and Moffitt (1984). We consider both retiree health insurance in general
and continuation benefits more specifically. Figure
4.1
shows
the
budget con-
straint facing an older worker between the ages of
55
and
65.
The horizontal
axis represents
the
age of retirement. The vertical axis measures the certainty
equivalent
(CE)
of consumption from age
55
onward.
This
differs from the
earlier literature, which has typically considered the relationship between the
age at retirement
and
the actual level of future consumption rather than the
CE
of future consumption.
This
departure is necessitated by our focus on the effect
of insurance coverage.
We assume that workers receive health insurance on their current job but
that they may or may not have retiree health insurance coverage. Firms that
provide postretirement health insurance do
so
on the same basis for both work-
ers and retirees, and these benefits cease upon eligibility for Medicare." We
also assume that once workers leave their current job, they will remain retired
for the rest of their life.
To
simplify the analysis, we ignore the effects of both
11.
In reality, most retiree health insurance plans do "top
off"
Medicare to some extent. This
does not alter the main conclusions
of
this section.

127
Health Insurance and Retirement
Cer
to
i
nty
Eq
u
iv
a
I
en t
of
Future
Consumption
65
R3 R4
*o
R*
55
Retirement
Age
Fig.
4.1
Modeling the effect
of
continuation coverage on retirement
Social Security and pensions; they could, however, be easily incorporated into
the analysis.
In the model, as in the real world, workers who retire without health insur-
ance coverage have two options: they may purchase an individual policy, or
go uninsured. In either case their out-of-pocket medical expenditures will be
significantly higher than if they receive retiree coverage or have the option of
continuing their group coverage. For a worker with retiree health insurance,
the slope of the budget constraint will be the after-tax wage, which is depicted
by line
AB
in figure 4.1. Since medical expenditures are insured, there is
no
uncertainty about future consumption.
For the worker without retiree coverage, the relative position and slope of
the budget constraint depend on two factors. First, because individuals are
risk
averse, those without retiree health insurance will have a lower level of
CE
consumption; this places the no-health-insurance budget constraint below that
of an insured worker.'* Second, because both the mean and the variance
of
medical expenditures rise with age, a year of health insurance coverage is
worth more at older ages. The cumulative reduction in
CE
consumption will
be greater at younger retirement ages, but the incremental effect will be
smaller. This latter effect gives curvature to the no-health-insurance budget
constraint, line
CD
in figure 4.1. At age
65
there is a jump
in
the no-health-
insurance budget constraint as Medicare equalizes the opportunities of all indi-
viduals.
If leisure is a normal good, retiree health insurance will lead to earlier retire-
ment, at age
R,
<
R,,
because such coverage makes individuals wealthier. As
12.
Risk aversion
in
this
model
operates in a
similar
fashion
to
higher
expected
medical
costs.

128
Jonathan
Gruber
and Brigitte
C.
Madrian
individuals are more risk averse, the wealth effect will increase as both the
level of the no-health-insurance budget constraint falls and its slope becomes
steeper.
Now consider the effect of a continuation coverage mandate that provides
one year of subsidized insurance coverage relative to having no health insur-
ance. For the risk-neutral worker, this is simply equivalent to an increment in
wealth equal to expected medical costs for a year minus the cost of the group
policy.13 This increment rises in value as the worker ages, since expected medi-
cal expenditures increase with age. Thus, the budget constraint with a continu-
ation coverage option, line
EE
lies above the no-health-insurance constraint
but below the retiree-coverage constraint. At younger ages, it is very close to
the no-health-insurance constraint; at age 64, it differs from
the
retiree-
coverage constraint by the cost of
the
group coverage. As workers become
more risk averse and the no-health-insurance constraint becomes steeper, the
distance between the no-health-insurance and the continuation coverage con-
straints will increase, and
this
increase will be greater at older ages. In this
case the value of one year of coverage will equal expected medical costs minus
the cost of the group policy plus the increase in
CE
consumption implied by
eliminating uncertainty in that year.
The value of both retiree health insurance and continuation benefits will rise
with the cost of being uninsured or the cost of buying individual insurance
in
the
private market. The important difference between these two sources of
coverage, however, is their age patterns: while retiree insurance coverage is
of
highest value to very early retirees, continuation benefits
are
more valuable at
older ages. Because of this, we might expect continuation benefits to be used
primarily by older workers seeking a “bridge to Medicare,” which allows them
to retire a certain number of months before age 65 without losing group cover-
age. If this is the case, we would expect the effect of continuation coverage on
retirement to be greatest at older ages.
There are, however, a number of complications that cloud this basic intu-
ition. The first is the empirical violation of one of our assumptions, namely,
that retirement is permanent. Diamond and Hausman (1984) report substantial
reentry rates for early retirees; among 55-64-year-olds, the one-year reentry
rate is approximately 15%. Sueyoshi (1989) finds that one-third of the elderly
“partially retire,” moving from permanent employment to less than full-time
work.
To
the extent that continuation coverage mandates facilitate movement
across jobs, rather than permanent retirement, they may have larger effects at
younger ages than was depicted above.I4
In this analysis we have assumed that retiree health insurance offers pure
13.
Once again, this amount is presumably positive even for a risk-neutral worker due
to
cross-
14.
One important consideration,
of
course,
is
whether this reentry
is
to jobs that offer health
subsidization
of
the group policy by younger coworkers.
insurance; unfortunately, there
is
little evidence on this question.

129
Health Insurance and Retirement
rents to workers in the firms that offer this type of coverage. In labor market
equilibrium, presumably at least a portion of these rents will be reflected in
lower wages for workers with retiree coverage. The extent to which these com-
pensating differentials offset the benefits of retiree health insurance at each
age will be a function of the employer’s ability to set relative age-specific
wages freely,I5 the mobility of workers across firms at different ages, and the
excess of the cost of continuation benefits over the group premium paid by the
early retiree.I6 The existence of compensating differentials may affect both
the location and the shape of the budget constraint facing the potential retiree;
the net effect on retirement age will
be
a function of the nature of the compen-
sating differential.”
Finally, we have ignored the possibility that workers may be liquidity con-
strained in making their retirement decisions. The fact that most retirees have
few liquid assets (Diamond and Hausman 1984) implies that such liquidity
constraints may
be
empirically important in determining retirement dates. This
explanation is suggested in both Diamond and Hausman (1984) and Burtless
and Moffitt (1984) in their discussion of why Social Security benefits do not
seem to affect retirement until they actually become available at age
62.
Sam-
wick (1993) finds that much of the estimated increase in retirement probabili-
ties attributed to Social Security occurs among those with pensions, suggesting
that all workers would like to take advantage of these benefits early, but that
only those with pensions can afford to do
so.
The presence of liquidity con-
straints could increase the effect of continuation benefits at younger ages, as
the wealth increment that these benefits represent could be loosening these
constraints.
4.4
Data and Regression Framework
4.4.1 Data
The data for
this
study must meet two key criteria. First, in order to exploit
the variation in state and federal continuation coverage legislation, they must
extend over a number of years before and after 1986. Second, there must be a
15. See Rosen (1986) for a discussion
of
the theory of compensating differentials. Gruber
(1994a) provides some evidence that shifting the costs of employer-provided benefits
to
distinct
demographic groups
in
the workplace is feasible.
16. Huth (1991) reports that
the
health insurance claims
of
COBRA
recipients exceed those of
active employees by
50%.
This difference in cost is attributed
to
adverse selection; it is the sickest
individuals who will find continuation coverage most attractive, and they will therefore be the ones
most likely to take it up. Similar evidence is provided in Long and Marquis (1992).
17. For example, if the entire cost of the benefits is shifted to older workers,
this
will lower the
slope of the budget constraint with continuation benefits (fig.
4.1)
relative to the budget constraint
without benefits (because wages for those with benefits fall), which will have both income and
substitution effects on the retirement decision.

130
Jonathan Gruber and Brigitte
C.
Madrian
large sample size
so
that the effects of state-law changes on older workers can
be identified. The data that best meet these two criteria are the Merged Outgo-
ing Rotation Group (MORG) sample of the
CPS.
The
CPS
is a nationally rep-
resentative survey that interviews over fifty thousand households each month.
The MORG file contains information on demographic characteristics and labor
force attachment during the survey week for one-quarter of each month’s
sample for each month of the year. This is the largest available annual data set
on individual labor force behavior in the United States.
Recent studies of retirement behavior have focused on dynamic modeling of
the transition into retirement. In this paper we instead use a static model of
whether or not an individual is currently retired, since the only labor force
information we have in the MORG is for the week of the interview. Evidence
on the stock of retired persons can still be useful for considering the effect of
continuation coverage mandates
on
retirement; if the laws are affecting flows,
they should affect stocks as well.L8 Furthermore, dynamic modeling strategies
for retirement decisions using survey data sets often suffer from an important
econometric difficulty, known as dynamic sample selection bias (Diamond and
Hausman
1984).
In the case of continuation coverage laws, this bias arises
from the fact that the set of individuals observed actually working after the law
has been in place for a number of years would be less likely to retire in re-
sponse to the law than would the entire population, because those most likely
to respond will have already retired. When the sample is selected on the basis
of those who are still working, the results will therefore be biased against
find-
ing an effect of the law.19 In a multivariate setting, the bias cannot be signed
a priori, and with time-varying covariates in the model, such as months of
continuation coverage, it is impossible to correct for this “left-censoring.”20
Our static regressions, which include all 55-64-year-old males regardless of
initial work status, do not suffer from this bias.
On the other hand, the major disadvantage of our static framework is that
we cannot control for the characteristics of
the
job from which the individual
has retired. This will be important if, for example, there is a systematic correla-
tion between the passage of these mandates and the nature of the jobs in the
states where they are passed. In the regression analysis we attempt to reduce
any bias that results from this potential correlation by controlling for the time-
18.
This
is not strictly true if the mandates affect the number
of
persons who decide to work at
all; in this case, both the numerator and denominator of the labor force participation rate would
be increasing, and the effect on
the
stock would be ambiguous.
This
is not likely to be a problem
for the sample of older males on which we focus.
19.
An
alternative way to see
this
point is to imagine a law that applied to a cohort rather than
to
an
age group. The individuals who are most likely to respond to
this
law will do
so
in the
first
year. In the next year, by selecting on the set of individuals who have not yet retired, we will bias
the results against finding an effect of the law. When the law applies to an age group, rather than
a cohort, this effect is attenuated by the fact that new members arrive into the age group.
20.
It
is
possible, however, to test for the magnitude of the bias; see Gruber and Madrian
(1995).

131
Health Insurance and Retirement
invariant characteristics of the states that pass these mandates. In section 4.5
we will contrast our findings from this static regression with those from dy-
namic models that allow us to better control for the types of jobs held by indi-
viduals.
4.4.2 Regression Framework
We focus
on
two definitions of retirement: whether or not an individual re-
ports being retired, and whether or not an individual is out of the labor force.
Both are based on a
CPS
question that asks about the major activity in which
an individual was engaged during the week before the survey. The latter defini-
tion is useful because
retirement
may be a subjective term that takes on differ-
ent meanings for different individuals. These retirement definitions
are
clearly
problematic along at least two dimensions. First, we are unable to contrast the
effect of these regulations on both “full” and “partial” retirement, as is done in
Burtless and Moffitt (1984) or Sueyoshi (1989). Second, we are unable to ac-
count for reentry into the labor market, as discussed in Diamond and Hausman
(1984). Nevertheless, these measures should provide reasonable estimates of
the effect of continuation coverage mandates on the propensity of older work-
ers to remain employed.
Our sample consists of men between the ages of
55
and 64. Overall,
20%
of
the sample report being retired, and
35%
are out of the labor force. The average
level of education is twelve years, and 9.5% of the sample is nonwhite.
We estimate the following probit model of retirement:
(1)
Pr(Retired,,)
=
@(a
+
p,*X,,
+
&*Statej
+
&*Timer
+
p,*Lawjr),
where
i
indexes individuals,
j
indexes states, and
t
indexes time.
Xi,,
is a set of
individual demographic characteristics,
Statej
is a set of state dummies,
Time,
is
a
set of year and month dummies, and
Lawjr
is the number of months of
continuation coverage available in state
j
at time
t?
The state fixed effects
control
for
any time-invariant characteristics
of
a state that may be correlated
with the state’s propensity to pass continuation coverage legislation. We in-
clude a set of year dummies to control for national trends in retirement behav-
ior that may be correlated with the passage of these laws, and month dummies
to control for seasonal patterns in retirement behavior. Thus, the effect of the
laws is identified in this model by changes in retirement behavior in states that
passed the laws (or that were affected by the federal law), relative to those
that did not, during the period after the laws were passed. Further identifying
variation comes from differences across states in the number of months of
21.
We
exclude individuals from two
states
from
our
sample: Hawaii, which has mandated
health insurance for
all
employees, and West Virginia,
for
which we were unable to definitively
date
the effective date of their continuation coverage mandate.

132
Jonathan
Gruber
and Brigitte C. Madrian
eligibility that these laws allow. Since we have monthly data, we phase in the
federal law in twelve equal increments between July 1986 and June 1987.
4.5
Results
The basic regression results are reported in table 4.9. The first column re-
ports the probit coefficients
from
the self-reported retirement equation, while
the second column gives the marginal probabilities implied by these coeffi-
Table
4.9
The Effect
of
Continuation Coverage on the Probability
of
Being Retired
Definition
of
Retired
Report Being Retired Not in the Labor Force
Marginal
Independent Variable Coefficient
Probability
Months
of
coverage
0.0036 ,0107
Married
-
0.0
154
-
.0037
Education
-0.0655
-.0162
(.0017)
(.0010)
(.0092)
(.0121)
(.0503)
(.0502)
(.0501)
(.0499)
(0498)
(.0496)
(.0496)
(.0494)
Nonwhite
-0.1204
-
,0282
55
years old
-
1.205
-.1950
56
years old
-
1.097 -.1853
57
years old
-1.016 -.I770
58
years old
-
0.925
1
-.1669
59
years old
-0.8115
-.1525
60
years old
-0.6254 -.1254
61
years old
-0.4903 -.lo24
62
years old
-0.0854
-
,0203
63
years old
0.1033 ,0260
64
years old
0.1938 .0504
(.0494)
(.0494)
Marginal
Coefficient Probability
0.0025
(.0015)
(.0009)
-0.3427
(.0081)
0.0918
(.0104)
0.1180
(.0443)
0.1935
(.0443)
0.2435
(.0443)
0.3157
(.0442)
0.4094
(.0442)
0.5302
(.MI)
0.6394
(.0442)
0.9977
(.0441)
1.161
(.0442)
1.262
(.0442)
-0.0577
.0098
-.0187
-.1173
,0305
,0392
,0646
,0816
,1063
,1385
,1804
,2187
,3441
,3996
,4324
Notes:
The table gives estimates from a probit equation
for
whether
or
not an individual is retired,
using data from the
1980-90
Merged Outgoing Rotation Groups of the Current Population Survey.
The sample comprises
214,508
men aged
55-64.
Coefficients for year, month, and state dummies
are not reported. Standard
errors
are in parentheses.

133
Health Insurance and Retirement
cientsZ2 The same is done in the third and fourth columns, using “not in the
labor force” as the definition of retirement. More education is associated with
a slightly lower probability of being retired and a much lower probability of
being out of the labor force. Being nonwhite is associated with a lower proba-
bility of retirement but a significantly higher probability of being out of the
labor force. Individuals who are married are less likely to be either retired or
out of the labor force. The age pattern of retirement propensities is familiar
from the previous literature; there is a large jump in the probability of being
retired at age
62,
and individuals aged 64 are
25%
more likely to be retired
than individuals aged
55.
This pattern is even more pronounced for being out
of the labor force, as the probability at age
64
is 40% greater than the probabil-
ity at age
55.
The availability of continuation coverage has a sizable and significant effect
on the probability of being retired. One year of coverage raises the probability
that an individual is retired by
1.1
percentage points, which is 5.4% of the
baseline probability of being retired in this sample. For the not-in-the-labor-
force regressions, the estimated effect of a year of continuation coverage is of
approximately the same magnitude as in the retired equation (although the
coefficient is only significant at the
10%
level), and suggests an increase in the
baseline probability of being out of the labor force of
2.8%.
The model described in section 4.3 suggests the possibility that the effect of
continuation coverage mandates on retirement could vary with age; intuitively,
it seemed that this effect should be strongest at older ages. In table 4.10, there-
fore, we free up the effect of months of continuation coverage by age. The
second and fifth columns present the marginal probability derivatives of the
probits. The third and sixth columns express these percentage-point increases
in retirement propensities as a fraction of the baseline retirement rate at each
age. This allows for a more natural interpretation of the percentage effects of
continuation benefits
on
retirement at each age.
In both equations the coefficients rise with age and are statistically signifi-
cant at ages
62
and above. The pattern of effects as a fraction of baseline retire-
ment probabilities, however, is not uniformly supportive of the hypothesis sug-
gested in section 4.3. For the retirement equation, there is actually a declining
pattern
of
effects by age; for the not-in-the-labor-force equation, the effects
are slightly increasing with age.
There are several possible explanations for this counterintuitive finding that
the effects are not proportionately greatest at the ages near Medicare eligibility.
22.
For dummy variables, the marginal probabilities are calculated by predicting the probability
of retirement with the dummy equal to one for the entire sample, predicting the probability with
the dummy set equal
to
zero for the entire sample, and taking the average
of
the difference in these
predictions across all individuals. For continuous variables, the marginal probability is calculated
by predicting the probability at the current level of the variable, predicting the probability by
adding one to the variable, and once again taking the average of the difference in these predictions
across individuals. The marginal probability on months of coverage is the probability increase
associated with going from zero to twelve months of coverage.

134
Jonathan
Gruber
and
Brigitte
C. Madrian
Table
4.10
The Age-Specific Effect
of
Continuation Coverage on the Probability
of
Being Retired
~ ~~
Definition of Retired
Report Being Retired
Not in the Labor Force
Marginal Percentage Marginal Percentage
Independent Variable Coefficient Probability of Baseline Coefficient Probability of Baseline
55*months ,0028 ,0083 13.3 .0012 0047 2.4
(.0023) (.0019)
56*months .0013 ,0037 4.8 ,0022 ,0088 4.1
(.0023) (.0019)
57'months ,002
1
.0061 6.8
-.0005
-.0021 0.9
(.0022) (0019)
%*months ,0027
,0080
7.6 .003
1
1.2
(.0022) (.0019)
59*months ,0046
.O
135 10.6 ,0019 .0074 2.6
(.002
1)
(.0019)
60*months .0024 ,007
1
4.2 .0018 ,0069 2.1
(.0021) (.0018)
6
1
*months ,0020 .0060 2.9
,002
1 ,0085 2.3
(.0020) (.0018)
62*months .0048 ,0143 4.2
,0040
,0161 3.2
(.0020) (.0018)
63*months
,0041
.0121 2.9 ,0045
.O
179 3.2
(.0020)
(.0018)
64*months ,0067 ,0202 4.5 .0063 ,025
1
4.1
(.0020) (.0018)
Notes:
The table gives estimates from a probit equation for whether
an
individual
is
retired, using data
from the 1980-90 Merged Outgoing Rotation Groups of the Current Population Survey. The sample com-
prises 214,508 men aged 55-64. Coefficients for year, month, age, and state dummies are not reported.
Education, race, and
marital
status are
also
included. Standard errors are in parentheses.
The first is the set
of
theoretical issues we raised in section
4.3,
such as the
possibility that individuals may face liquidity constraints that are loosened by
this temporary health insurance. The second reason is statistical: we may not
have enough power to these probits to distinguish true larger effects at older
ages from the effects at younger ages. Given the precision of our estimates, this
seems an unlikely explanation for the unexpected age pattern
of
our results.
Alternatively, it may be that our result is spurious. One potential problem
with our identification strategy is that the passage of these laws could be corre-
lated with some other change
in
retirement behavior in these states. Alterna-
tively, it could be that the laws themselves are endogenous responses to
changes
in
retirement propensities among the population; that is, if more indi-
viduals are retiring, states may respond by mandating benefits that cover indi-
viduals after their retirement.
One form of potential endogeneity could be that the propensity of legisla-

135
Health Insurance and Retirement
tures to mandate continuation coverage is correlated with long-term within-
state trends in retirement behavior. In this case, even with state fixed effects
included in the regression, there will be a spurious correlation between
changes in retirement behavior within a state and the passage of a continuation
coverage mandate. One possible control for such spurious causation is to in-
clude in the regression not only state effects but state-specific trend terms; that
is, we interact each state effect with a trend for the ten-year period.23 The re-
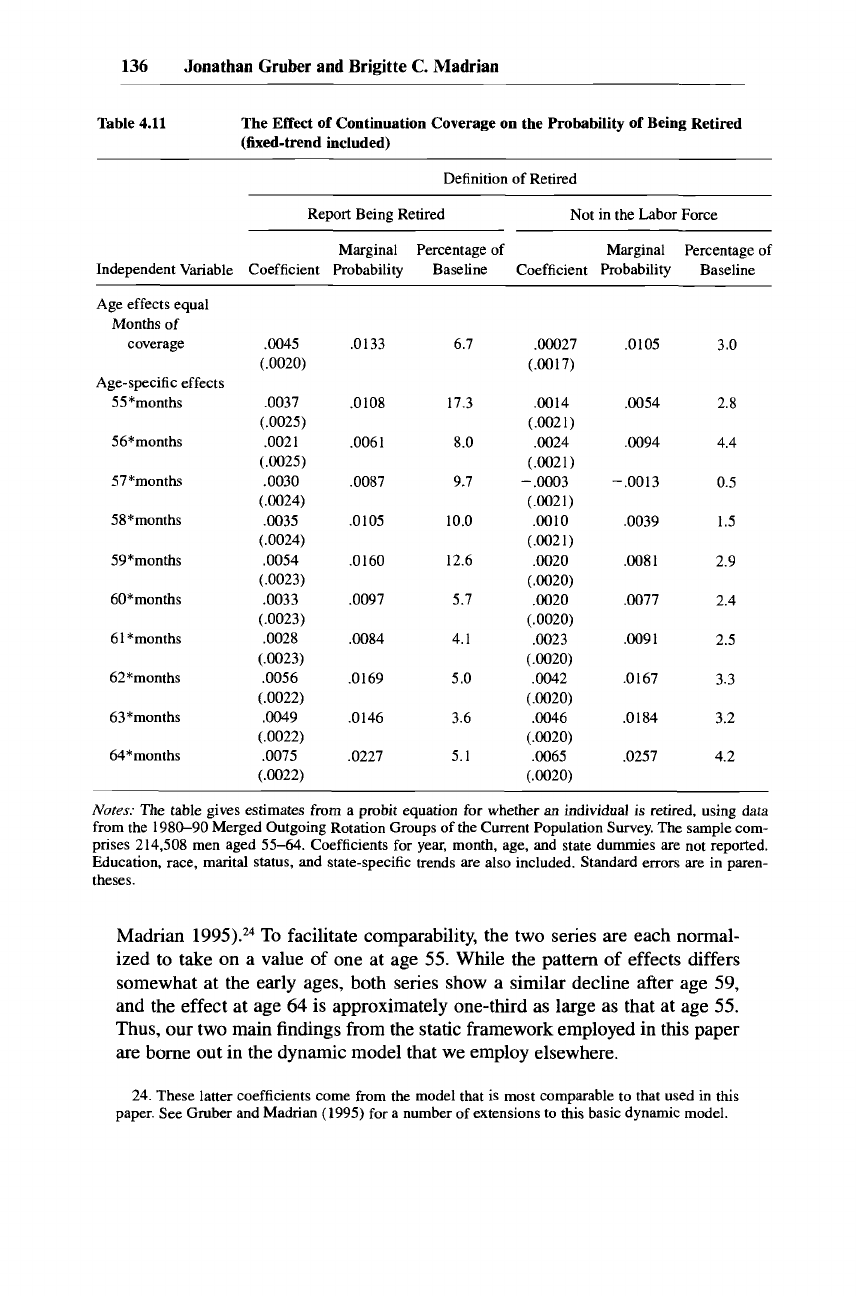
sults from this specification check are presented in table 4.11. For the not-in-
the-labor-force regression, the age-specific coefficients are virtually un-
changed from those in table 4.10; in the retirement equation, the coefficients
are slightly larger, but once again the effects are very similar.
A
further potential problem with these findings is that it may not be appro-
priate to compare the effects of the state and federal mandates.
As
we noted
earlier, these mandates differ along a number of dimensions, the most im-
portant being that the state mandates do not apply to self-insured firms, while
the federal mandate does not apply to small firms. In results not reported, we
have rerun these regressions for the period prior to July 1986 in order to restrict
our analysis to the effects of the state laws. The results are somewhat stronger
than those in tables 4.10 and 4.11, although the age patterns are similar.
In
related work (Gruber and Madrian 1995), we consider the effect of con-
tinuation benefits on transitions into retirement using two different data sets-
the March files of the
CPS,
and the Survey of Income and Program Participa-
tion
(SIPP).
These data sources allow us to estimate dynamic retirement mod-
els and to control for some characteristics of the jobs from which individuals
retire. The sample sizes are much smaller than we have with the MORG data,
however, and we are confronted with the issue of dynamic sample selection,
discussed above. Nevertheless,
this
study confirms the two key findings of the
research reported above. First, there is a sizable and significant effect of contin-
uation coverage on retirement behavior. Using one-year retirement transitions
in the March
CPS,
we find that one year of continuation coverage raises retire-
ment propensities by 1.4 percentage points. This is quite similar to the 1.1
percentage-point effect estimated in this paper using the MORG data. Further-
more, the implied effect on the hazard rate in both the March
CPS
and SIPP
data is identical.
Second, despite the presumption that these laws should act as a “bridge to
Medicare,” the estimated effects in these dynamic models do not rise with age
either. Figure 4.2 graphs the change in the propensity to be retired from having
a year of continuation coverage estimated from the MORG regressions (col-
umn three of table 4.10) along with the percentage increase in retirement prob-
abilities estimated using transition data from the March CPS (Gruber and
23.
The trend
is
monthly, taking on values
of
1
to
132.
This
type
of
“random growth” or “fixed
trend” estimator
is
suggested
by
Heckman and
Hotz
(1988) and is used by Jacobson, LaLonde,
and Sullivan (1992) and Gruber (1994b).
136
Jonathan Gruber and Brigitte
C.
Madrian
Table
4.11
The Effect
of
Continuation Coverage
on
the Probability
of
Being Retired
(fixed-trend included)
~~
Definition of Retired
Report Being Retired Not in the Labor Force
Marginal Percentage of Marginal Percentage of
Independent Variable Coefficient Probability Baseline Coefficient Probability Baseline
Age effects equal
Months
of
coverage
Age-specific effects
55*months
56*months
57*months
58*months
59*months
60*months
6
1
*months
62*months
63 *months
64*months
,0045
(.0020)
.0037
(.0025)
,002
1
(.0025)
.0030
(.0024)
,0035
(.0024)
,0054
(.0023)
.0033
(.0023)
,0028
(.0023)
,0056
(.0022)
,0049
(.0022)
,0075
(.0022)
,0133 6.7
,0108 17.3
,006 1 8.0
,0087 9.7
.0105 10.0
.O
160 12.6
,0097 5.7
,0084 4.1
.O
169 5.0
.O
146 3.6
.0227 5.1
.OOO27
(.0017)
,0014
(.0021)
,0024
(.0021)
-
,0003
(.0021)
.0010
(.0021)
.0020
(.0020)
.0020
(.0020)
.0023
(.0020)
.0042
(.0020)
,0046
(.0020)
,0065
(.0020)
,0105 3.0
.0054 2.8
,0094 4.4
-.0013
0.5
,0039
1.5
,008
1
2.9
,0077 2.4
,009
1
2.5
,0167 3.3
,0184 3.2
.0257 4.2
Notes:
The
table gives estimates
from
a probit equation
for
whether
an
individual is retired, using data
from the 1980-90 Merged Outgoing Rotation Groups of the Current Population Survey.
The
sample com-
prises 214,508 men aged
55-64.
Coefficients for year, month, age, and state dummies are not reported.
Education, race, marital status, and state-specific trends are also included. Standard errors are in paren-
theses.
Madrian
1995).24
To
facilitate comparability, the two series are each normal-
ized to take
on
a value of one at age
55.
While the pattern of effects differs
somewhat at the early ages, both series show a similar decline after age
59,
and the effect at age
64
is approximately one-third as large as that at age
55.
Thus, our two main findings
from
the static framework employed in
this
paper
are borne out in the dynamic model that we employ elsewhere.
24. These latter coefficients come from the model that
is
most comparable
to
that used in this
paper. See
Gruber
and Madrian (1995) for a number of extensions to
this
basic dynamic model.

137
Health Insurance and Retirement
1.6
I
1.4
1.2
1
0.8
0.6
0.4
0.2
nl
I
I
I I I
I
I
I
L
1
55
56
57 58 59
60 61 62 63 64
Age
March
CPS
-
_________________
MORG
Fig.
4.2
Relative age-specific effects
of
continuation coverage
on
retirement
It is also interesting to consider what the magnitude of these findings imply
about individual valuation of continuation benefits by comparing them to the
estimated increase in retirement propensities following an increase in postre-
tirement income. The results from a static probit model of retirement in Sam-
wick (1993) suggest that a
$5,000
increment
to
Social Security wealth in-
creases the retirement hazard by approximately
8%.
In a stochastic dynamic
programming model employed by Stock and Wise (1990a, 1990b) and Lums-
daine, Stock, and Wise (1992, 1994), they find that a
$5,000
increase in the
value of pension wealth leads to an increase in the retirement hazard of be-
tween
10
and 13% for individuals between the ages of
55
and
64.25
The
basic specification of Gruber and Madrian (1995) finds that one year
of
continuation coverage raises the retirement hazard by 32%. This implies that a
year
of
continuation benefits is valued at between
$12,300
and
$15,000
in
terms of postretirement wealth. Based on the cost information reported in sec-
tion
4.2,
a COBRA policy would save an older worker approximately
$4,500
per year on the price of family coverage. Taken at face value, these results
suggest that workers value the insurance received from continuation coverage
policies at a somewhat higher level than its associated cost savings. This may
reflect the fact that the individual policy we priced, as with most individual
policies, excluded preexisting conditions for some period. Alternatively, it may
be that a number of early retirees must pay substantially more for individual
policies or are unable to obtain such policies at
all.
25.
We are grateful
to
Andrew Samwick, Robin
Lumsdaine,
and
James Stock for
performing
these calculations
for
us.

138
Jonathan Gruber and Brigitte
C.
Madrian
4.6
Insurance Coverage
In this section we consider the effects of continuation coverage mandates on
the insurance coverage of early retirees. If continuation coverage mandates are
having an effect on the retirement decisions of older workers, then, by defini-
tion, they should be affecting their insurance coverage as well. Thus, evidence
that such mandates increase insurance coverage among early retirees provides
a necessary (but not sufficient) specification check of
our
result that these man-
dates affect retirement behavior. Furthermore, it is interesting to contrast the
direct effects of these mandates on insurance coverage with their indirect ef-
fects
on
retirement behavior.
To
what extent do continuation coverage man-
dates affect the "inframarginal" individual, who would have retired in their
absence, relative to the "marginal" individual whose retirement decision is
made in response to their presence?
In order to investigate the effect of continuation coverage mandates on insur-
ance coverage, we use data from the
SIpP.26
The SIPP is a nationally represen-
tative survey of households designed to collect information on the economic
and demographic characteristics of individuals and their families. We use data
from the
1984,1985,1986,
and
1987
panels of the
SIPP.
Sample members are
interviewed every four months for roughly two and a half years and asked to
provide information about their labor market activity, income, and participa-
tion in welfare and transfer programs over the previous four months. The first
interviews
of
the
1984
panel were conducted in October
1983,
while the initial
interviews for subsequent panels commenced in February of the corresponding
calendar year. For previously cited reasons, we exclude individuals living in
West Virginia and Hawaii. We also drop individuals from several other small
states because, out of concern for confidentiality, the
SIPP
has grouped these
states together, thereby making it impossible to assign the appropriate state
laws to individuals in these states.27
We restrict our sample to men aged
55-64
who retired during the sample
period. The
SIPP
does not ask individuals directly whether they have retired.
We therefore use a measure of retirement based on length
of
time out of the
labor force. This has the advantage, relative to point-in-time self-reported mea-
sures, of capturing transitions to nonwork rather than partial (but perceived)
retirement. It has the disadvantage, however, of not allowing
us
to disentangle
retirement from other reasons for a temporary absence from the labor force.
Following Rogowski and Karoly
(1992),
we define retirement as a departure
26.
To
keep the sample of individuals comparable to the MORG data used in
this
paper, one
could in principle use the March
CPS
to
look
at insurance coverage over
a
similar time period.
Unfortunately, a
1988
change in the questionnaire that altered the reported coverage rates of older
individuals who were not working (precisely the group of interest) precludes performing a reliable
analysis with
this
data set.
27.
These states are Alaska, Idaho, Iowa, Maine, Mississippi, Montana, New Mexico,
North
Dakota, South Dakota, Vermont, and Wyoming. The
CPS
results are similar if we restrict
our
CPS
sample in the same fashion. See Gruber and Madrian
(1995)
for more detail on our
SIPP
sample.

139
Health Insurance and Retirement
Table
4.12
Continuation Coverage and the Probability
of
Being Insured
after Retirement
Independent Variable Coefficient
Marginal Probability
Married
,0820 ,026
Black
-
,8403
-
.293
Education
,0381 ,012
Age
.1788
-
,020
Age2
-.oO01
-
Months of coverage ,0163 ,005
(.1764)
(.2227)
(.0122)
(.0903)
(.00006)
(.0084)
Notes:
The table gives estimates of the probability of being insured after retirement, using data
from the Survey of Income and Program Participation. The sample comprises 527 men aged 55-64
who retired over the sample period. Coefficients for industry and occupation dummies are not
reported. Standard errors are in parentheses.
from the labor force of five or more months.z8 Individuals who are not in the
labor force for at least the first four months for which we observe them are
excluded from the sample, and individuals who report being out of the labor
force in the last five months of the panel are censored at the last month for
which they are in the labor force.
Table 4.12 presents the results from a probit equation for whether or not an
individual is covered by employer-provided health insurance after retirement.
The key independent variable is the number of months of continuation cover-
age available at the time of retirement. The results suggest that an extra month
of continuation coverage increases the probability of being insured after retire-
ment by
0.5%.
This
implies that one year of coverage would increase the proba-
bility of being insured by
6%,
while eighteen months would increase the prob-
ability of coverage by 9%,
a
result consistent with that found by Rogowski and
Karoly (1992). The results of table 4.12 corroborate the evidence
on
take-up
rates presented in section 4.2.
As
mentioned, Zedlewski (1993) estimates that
5.2% of retired individuals between the ages of 55 and
64
are covered by
COBRA.
This fraction is very similar to our
6%
estimated increase in coverage
from one year of continuation coverage, which is the average length of time
for which older individuals receive
COBRA
(Flynn 1992).
28. Rogowski and Karoly (1992) actually impose a six-month rule for departure from the labor
force. It
turns
out that almost all
of
the
individuals who are out of the labor force for five months
are actually out for
six
or more months.
This
definition of retirement helps alleviate the problem
of measurement error in the reporting of individual labor force status; since individuals are inter-
viewed every four months, they must report that they are out of the labor force in two consecutive
interviews
to
be
counted
as
retired. See Gruber and Madrian (1995) for further discussion.

140
Jonathan Gruber and Brigitte
C.
Madrian
Furthermore, we can reconcile
this
finding with our estimates of the effect
of continuation coverage mandates on retirement. Our findings imply that one
year of coverage raised the probability of being retired by about
1.1
percentage
points, but that it raises the probability of being insured by
6
percentage points.
This suggests that the primary effect of these mandates is “inframarginal.” That
is, they provide insurance coverage for individuals who would have retired in
the absence of these mandates even though they would not have been covered
by employer-provided health insurance. Thus, continuation coverage mandates
may be policies with a sizable bang for the buck: they have a large and signifi-
cant effect along their intended dimension, increased insurance coverage, with
a relatively small effect along their unintended dimension, increased re-
tirement.
4.7
Conclusion
A
number of current policy proposals in the United States, such as increas-
ing the age of Medicare eligibility to
67
or providing guaranteed health insur-
ance coverage for all citizens, would affect the health insurance coverage of
early retirees. Thus, it seems especially important at this time to understand
the interaction between insurance coverage and the retirement decision. If re-
tirement is very sensitive to insurance coverage, for example, it could have
important public finance implications for policies that provide universal health
insurance coverage; a spate of retirement may nontrivially lower the tax base
on which new policies can be financed.
Our strategy for estimating the effect of health insurance on retirement has
been to examine the effect of state and federal continuation coverage mandates
on retirement propensities. We do this in a static regression framework, which
allows us to exploit a very large data set and to avoid the problems of dynamic
sample selection that plague other studies based on survey data. Our results
suggest that continuation coverage mandates have a sizable and significant ef-
fect on retirement. Contrary to our basic intuition, however, the effects are not
necessarily the strongest at older ages. Rather, taken in conjunction with evi-
dence from dynamic models, we appear to find declining effects by age. We
also found that one year of continuation benefits is associated with a
6%
in-
crease in insurance coverage levels, suggesting that these policies are not only
inducing retirement, but are “inframarginally” covering those who would have
retired anyway.
Our use of continuation coverage regulations as the source of variation for
identifying the effect of insurance coverage on retirement has both advantages
and disadvantages relative to looking directly at workers with and without
employer-provided retiree health insurance. One potential problem with the
latter strategy is that the researcher is unable to control for job characteristics
that may be correlated with both the generosity of retiree health coverage and
the
incentives that these
jobs
offer for retirement.
An
obvious example is

141
Health Insurance
and
Retirement
pensions (which are accounted for in both Lumsdaine, Stock, and Wise
1994
and Gustman and Steinmeier
1994).
There may be a number of other ways in
which firms encourage or discourage retirement, however, such as through
the tasks that they assign older workers or the wage profile that these workers
are offered. Furthermore, there may be sorting of workers by retirement pro-
pensities into the types of
firms
that do or do not offer retiree health insurance.
To
the extent that these are unobserved by the econometrician but correlated
with both the offering of retiree coverage and the retirement decision, they will
bias the estimated effect of such coverage on retirement. What is needed to
identify the effect of retiree health insurance is exogenous assignment of such
coverage to individuals that is independent of these other job characteristics.
Continuation coverage mandates potentially provide such exogenous as-
signment.
The primary disadvantage of our strategy is that continuation benefits are
more expensive
to
the early retiree than retirement health insurance and pro-
vide coverage only for a limited number of months. These differences may
make it unreasonable to extrapolate our results to infer the effects of full retiree
health insurance coverage. Future research should focus on combining a study
of true employer-provided retiree coverage with an identification strategy that
overcomes the omitted-variable bias problems described above.
References
Bazzoli, Gloria J. 1985. The Early Retirement Decision: New Empirical Evidence on
the Influence of Health.
Journal
of
Human Resources
20214-34.
Bound, John, and Timothy Waidmann. 1992. Disability Transfers, Self-Reported
Health, and the Labor Force Attachment of Older Men: Evidence from the Historical
Record.
Quarterly Journal
of
Economics
107:
1393-1420.
Burtless, Gary. 1986. Social Security, Unanticipated Benefit Increases, and the Timing
of Retirement.
Review
of
Economic Studies
53:781-805.
Burtless, Gary, and Robert A. Moffitt. 1984. The Effect
of
Social Security Benefits on
the Labor Supply of the Aged. In
Retirement and Economic Behavior;
ed. Henry J.
Aaron and Gary
Burtless.
Washington, DC: Brookings Institution.
Congressional Research Service.
1988.
Costs and Effects
of
Extending Health Insur-
ance Coverage.
Washington, DC: Library of Congress.
Diamond, Peter A., and Jerry A. Hausman. 1984. The Retirement and Unemployment
Behavior of Older Men. In
Retirement
and
Economic Behavioc
ed. Henry J. Aaron
and Gary Burtless. Washington, DC: Brookings Institution.
Employee Benefits Research Institute. 1990.
Employee Benejt Notes.
Washington, DC:
Employee Benefits Research Institute, November.
Farley, Pamela J. 1986.
Private Health Insurance in the United States.
National Health
Care Expenditures Study Data Preview 23, DHHS Publication (PHS) 86-3406.
Washington, DC: U.S. Department of Health and Human Services, National Center
for Health Services Research and Health Care Technology Assessment.
Flynn, Patrice. 1992. Employment-Based Health Insurance: Coverage under COBRA

142
Jonathan Gruber and Brigitte
C.
Madrian
Continuation Rules. In U.S. Department of Labor, Pension and Welfare Benefits Ad-
ministration,
Health Benejits and the Workforce.
Washington, DC: Government Print-
ing Office.
Gruber, Jonathan. 1994a. The Incidence of Mandated Maternity Benefits.
American
Economic Review
84:622-41.
.
1994b. State Mandated Benefits and Employer Provided Health Insurance.
Journal of Public Economics
55:433-64.
Gruber, Jonathan, and Brigitte C. Madrian. 1995. Health Insurance Availability and the
Early Retirement Decision.
American Economic Review
85.
Gustman, Alan L., and Thomas L. Steinmeier. 1994. Employer-Provided Health Insur-
ance and Retirement Behavior.
Industrial and Labor Relations Review
48236-102.
Hausman, Jerry A., and David A. Wise. 1985. Social Security, Health Status, and Retire-
ment. In
Pensions, Labol; and Individual Choice,
ed. David A. Wise. Chicago: Uni-
versity of Chicago Press.
Heckman, James, and
V.
Joseph Hotz. 1988. Choosing among Alternative Non-
Experimental Methods for Estimating the Impact of Social Programs: The Case of
Manpower Training.
Journal of the American Statistical Association
842362430.
Hewitt Associates. 1985.
Continuation
of
Group Medical Coverage: A Study
of
State
Laws.
Lincolnshire, IL: Hewitt Associates.
Hurd, Michael D. 1990. Research on the Elderly: Economic Status, Retirement, and
Consumption and Saving.
Journal of Economic Literature
28565-637.
Huth, Stephen A. 1991. COBRA Costs Average 150% ofActive Costs.
Employee Bene-
fit Plan Review
46:14-19.
Jacobson, Lewis
S.,
Robert J. LaLonde, and Daniel G. Sullivan. 1992. Earnings Losses
of Displaced Workers. Federal Reserve Bank of Chicago Working Paper 92-28. Chi-
cago: Federal Reserve Bank of Chicago.
Long, Stephen H., and M. Susan Marquis. 1992. COBRA Continuation Coverage:
Characteristics of Enrollees and Costs in Three Plans. In U.S. Department of Labor,
Pension and Welfare Benefits Administration,
Health Benejits and the Workforce.
Washington, DC: Government Printing Office.
Lumsdaine, Robin L., James H. Stock, and David A. Wise. 1992. Three Models of
Retirement: Computational Complexity versus Predictive Validity. In
Topics in the
Economics of Aging,
ed. David A. Wise, 19-57. Chicago: University of Chicago
Press.
.
1994. Pension Plan Provisions and Retirement: Men and Women, Medicare,
and Models. In
Studies in the Economics of Aging,
ed. David
A.
Wise, 183-220.
Chicago: University of Chicago Press.
Madrian, Brigitte C. 1994. The Effect of Health Insurance on Retirement.
Brookings
Papers on Economic Activity
1: 181-252.
Rogowski, Jeannette A., and Lynn A. Karoly. 1992. Retirement and Health Insurance
Coverage. In U.S. Department of Labor, Pension and Welfare Benefits Administra-
tion,
Health Benejts and the Workforce.
Washington, DC: Government Printing
Office.
Rosen, Sherwin. 1986. The Theory of Equalizing Differences. In
Handbook
of
Labor
Economics,
vol. 1, ed. Orley Ashenfelter and Richard Layard. Amsterdam: North-
Holland.
Samwick, Andrew A. 1993. The Joint Effect of Social Security and Pensions on the
Timing of Retirement: Some New Evidence. Massachusetts Institute of Technol-
ogy. Mimeo.
Stock, James H., and David
A.
Wise. 1990a. The Pension Inducement to Retire: An
Option Value Analysis. In
Issues in the Economics ofAging,
ed. David A. Wise. Chi-
cago: University of Chicago Press.

143
Health Insurance and Retirement
.
1990b.
Pensions, the Option Value
of
Work, and Retirement.
Econometrica
58
Sueyoshi, Glenn
T.
1989.
Social Security and
the
Determinants
of
Full and Partial Re-
tirement:
A
Competing Risks Analysis. NBER Working Paper
no.
31
13.
Cambridge,
MA: National Bureau of Economic Research.
Thompson Publishing Group.
1992.
Employers Handbook: Mandated Health Benejts:
The COBRA Guide.
Salisbury,
MD:
Thompson Publishing Group.
Zedlewski, Sheila R.
1993.
Retirees with Employment-Based Health Insurance. In
U.S.
Department
of
Labor, Pension and Welfare Benefits Administration,
Trends
in
Health
Benejits.
Washington, DC: Government Printing Office.
(5):
1151-80.
COInlllent
Richard J. Zeckhauser
Old workers who turn out the widget,
Here studied by Jon and by Brigitte,
Their fondest desire
Is
just to retire,
But the cost of health care makes them fidget.
Legislation attuned to their plight:
Makes twelve months’ insurance a right.
With the cost now reduced,
A
five-point-four percent boost
In retirement rate is in sight.
Jonathan Gruber and Brigitte Madrian’s carefully crafted article springs from
the observation that health insurance is a pricey commodity
for
individuals of
prime retirement age, due to adverse selection and transactions costs. Recog-
nizing this, a number of states, and recently the federal government, have
passed legislation requiring that companies sell continuing coverage to their
departing employees. The price can’t exceed the average employee’s cost, plus
a sliver. (The federal mandate now extends for eighteen months.)
Such coverage slashes the costs of health insurance. Not surprisingly, for
each year
of
mandated coverage
an
additional
6%
of retirees buy health insur-
ance. The dramatic reduction in health insurance costs also makes retirement
more attractive. Indeed, employing appropriate econometric wizardry, Gruber
Richard
J.
Zeckhauser is the
Frank
P. Ramsey Professor of Economics at the
John
F.
Kennedy
School
of
Government, Harvard University, and
a
research fellow of the National Bureau of
Eco-
nomic Research.

144
Jonathan
Gruber
and Brigitte
C.
Madrian
and Madrian (GM) infer that an additional
1.1%
of the 55-64-year-old cohort
choose retirement, which is 5.4% of its baseline value.’
The model implicit
in
figure
4.1
suggests that employees value the continued
coverage by the certainty equivalent of the difference between the price for the
extended insurance charge and a retiree’s other health coverage options-ei-
ther the selection-biased price of privately purchased insurance, or the highly
variable costs of self-insurance. Since
this
difference grows as people get older
and sicker, and health becomes more heterogeneous, the retirement induce-
ment will grow with age.
GM
therefore predict that the older workers are, the
more mandates for continuation of health coverage will increase retirement as
a percentage of baseline. But they find the reverse.
GM might have made the opposite prediction if they had pushed the hetero-
geneity button a bit harder. Say potential retirees fall into two groups, Calibra-
tors and Instinctuals. The Calibrators are the tribe traditionally studied by
economists;2 they leave the Instinctuals to the sociologists. The Instinctuals
range from bon vivants, the silver-haired types pictured on a golf course in
national media advertising, to those too sick to work. One feature unites the
Instinctuals-their decision to retire is unaffected by the cost of health in-
surance.
Evidence on the incidence of illness by age, including some presented by
GM,
show a rapid acceleration with age. For this reason alone, we would ex-
pect many more Instinctuals to have retired at 64, say, than at
55.
Conceivably
the acceleration with age of Calibrators’ induced retirements could be more
than proportional to the Instinctuals’ upsweep. But maybe not. It depends in
part on the elasticity of Calibrators’ retirement with respect to health costs at
each age.
The curve showing the number of workers who will be induced to retire
by various levels of health savings may resemble many textbook labor-supply
curves, with a range that is relatively flat followed by a range that is fairly
inelastic. When coverage costs are reduced, the “cheap retirers” will
go
early.
And the escalation in benefits over time, as people get sicker, may not be suffi-
cient to get “expensive retirers” to participate. For example, it is often found
that companies’ early retirement plans disproportionately push out those at the
1.
The impact is actually greater than that, since many employers were presumably already
offering coverage before the government mandated it. As the mandate increases, it becomes a
binding constraint on
an
ever-increasing percentage of firms. Assuming all months of coverage
have the same effect, as GM do,
this
would produce a built-in nonlinearity.
2.
The Calibrators have quite a challenge, since the implicit calculations are quite complex,
probably sufficiently complex to defeat a pride of
NBER
researchers. GM find, for example, that
one year
of
continuation coverage saves a worker $4,500 and has the same retirement conse-
quences as
$17,000
in Social Security wealth. They conclude, with reservations about variability
among workers, that the two
are
worth the same. The logic doesn’t follow, since the former is a
price effect, whereas the latter is an income effect. Pity the poor worker confronted with this
problem. Amos Tversky might explain the worker’s behavior better than Alfred Marshall.

145
Health Insurance and Retirement
bottom end of the qualifying age range. And
so
it may be with some retirement
due to reduced health care costs.
Retirement is a complex decision, involving health, location, and friends, as
well as dollar costs and benefits, and we should be cautious before predicting
the age-specific effects of inducements. We should be more cautious still when
making predictions relative to baselines, given the array of reasons why work-
ers retire.
GM are moving on to dynamic assessments of the transition to retirement in
forthcoming work. They have already shown they can do the econometric nip-
ups required to deal with sample selection issues. A bit of dextrous modeling
as an accompaniment would now help them distill more about who retires
and why.
GM complement
an
informative compilation of background data-age-
specific patterns
of
health, expenditures, and coverage-with sound empirical
methods to reach intuitive results. Embracing these results, what shall we make
of mandates that require employers to sell health insurance to their retirees at
a subsidized price? The economist’s first concern-excess consumption-is
hardly a problem: rational retirees would buy the insurance even at fair actuar-
ial prices.
What
of
distributional consequences? Until wage adjustments work through
the system-which could take quite a while, given that the system shock is a
government mandate-these impositions represent a transfer from continuing
workers to retirees. In the long run, wages will be pushed down to pay for this
new mandated benefit, which thus becomes an imposed subsidy of one group
by another.
What are the welfare consequences of this imposed subsidy? Should rational
employers dealing with rational workers offer such coverage voluntarily? At
least to deal with the adverse selection problem, it might seem
so.
Subsidized
insurance is a second-best remedy to the hidden information problem. Add
to this the labor economist’s belief that age-earnings profiles are steeper than
productivity profiles, which implies that older workers don’t earn their keep.
A
subsidy for retirement may promote efficiency in the composition of a com-
pany’s labor force, quite apart from saving the company money.
The company should also be concerned about who decides to retire in return
for this small health coverage benefit. (The federally mandated eighteen
months saves the retiree roughly
$7,000,
but costs the company far less, since
it also subsidizes health coverage for older workers who do not retire.) If the
most talented workers, who are presumably underpaid given bureaucratic con-
straints at firms, dash to retire (perhaps due to confidence that they can get
another job), this will be poor policy. But if the sickly take off, reassured by
coverage for a period in retirement, it looks more promising. In any delibera-
tion by the firm, it should recognize, as GM find, that an extension of coverage
induces about
5.5
times as many people to buy insurance as it does to retire.

146
Jonathan Gruber and Brigitte
C.
Madrian
In the short run, this multiplies the cost enormously. In the long run, downward
wage adjustments wash out this effect. In sum, particularly in
an
era when
many established firms are downsizing, continued health coverage in retire-
ment may be an inexpensive way around a range of labor market rigidities.
What of the government’s interest in promoting health coverage continua-
tion? Some would argue that the government needs to step in due to market
imperfections in the insurance market for older workers. But firms already
have an incentive to address this problem on their own. The intensity of govern-
ment action in this area is probably due to a desire to provide a subsidy to a
specified group of workers-those about to retire-leaving till later the worry
about who will ultimately pay.
The government’s major concern should be whether we want workers to
retire. If you think the size of the labor force is relatively fixed, a popular but
noneconomic viewpoint, then you might promote retirement to spread things
around. An economist would urge the government to consider the relationship
of expected Social Security less taxes to retirement age. Since the relationship
is strongly negative, the government should be in the business of delaying, not
promoting, retirement.
These are revolutionary times in health insurance. Market conditions are
forcing firms to drastic action. The federal government may soon make dra-
matic moves. GM demonstrate that even comparatively modest changes in gov-
ernment health coverage regulations have significant effects on retirement be-
havior. Their paper offers a more general lesson: health insurance interventions
by the government have significant effects on the operation of labor markets.
